|
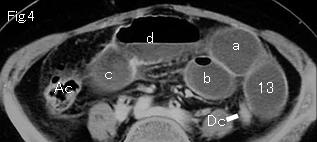
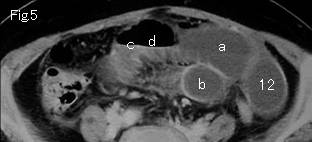
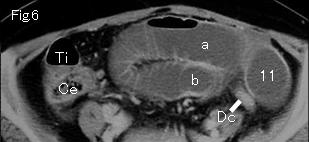
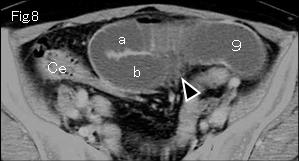
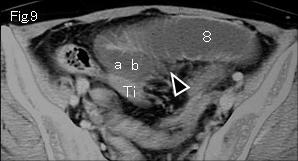
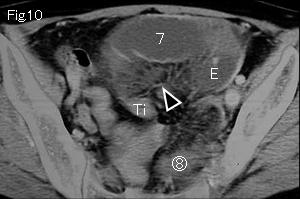
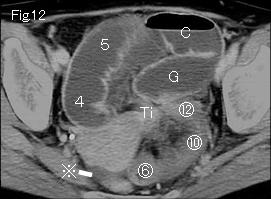
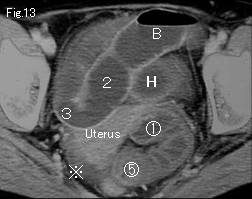
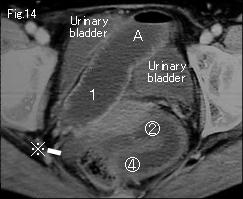
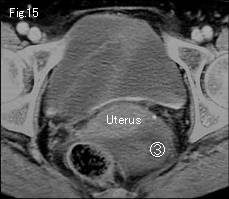
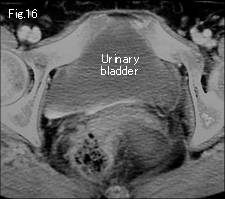
Ascending colon (Ac) and cecum (Ce) containing no liquid contents in Fig.4-Fig.6 suggest that distended small bowel indicate mechanical obstruction. Ti: Terminal ileum. Dc: Descending colon. The wall of distended small bowel demonstrates excellent contrast-enhancement indicating to be viable. They are gasless, mesenteric stranding (black arrowhead) is shown in Fig.8-Fig.11, and ascites (reference mark) is recognized in Fig.12-Fig.14, these 3 findings are characteristic of strangulated obstruction. On tracking down A of Fig.14, it occludes at H of Fig.13, and its caudal side continues to collapsed terminal ileum (Ti) of Fig.10-Fig.12. 1 of Fig.14 progresses in number order, and connects to 13 of Fig.4. ab of Fig.9 becomes a and b and ascend as shown. Consequently, the small bowel which was tracked down manifests simple obstruction occluding at H of Fig.13. There is slightly distended small bowel group in pelvis ( Fig.10-Fig.15), which represents strangulated obstruction. On tracking down, circle number 1 of Fig.13 and circle number 12 of Fig.12 are obstruction sites indicating closed loop formation. Closed loop close to uterus which is displaced to right side is suggestive of small bowel herniation through a defect of the broad ligament of uterus. The wall of closed loop manifests satisfactory contrast enhancement indicating viable bowel. Long ileus tube was inserted but the abdominal pain was not relieved over four days, and laparotomy was undertaken. Above findings were confirmed with 15cm viable herniated ileum at surgery.
|