|
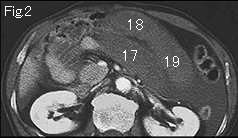
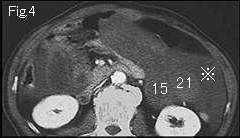
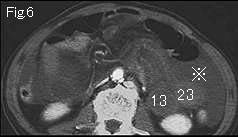
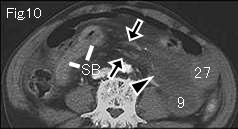
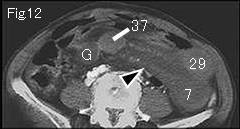
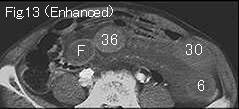
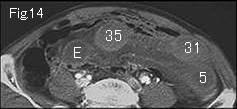
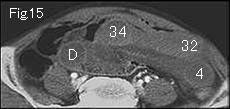
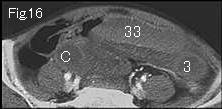
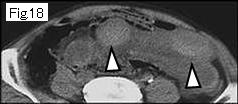
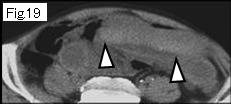
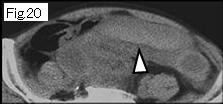
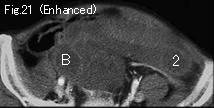
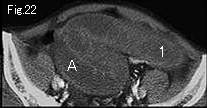
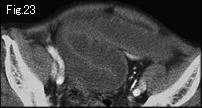
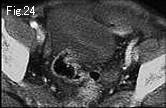
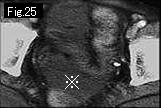
Distension limited to small bowel is suggestive of mechanical obstruction. There is a large quantity of ascites (reference mark of Fig.4-Fig.6) in left lateral gutter and pelvic cavity of Fig.25. Black arrowheads of Fig.9-Fig.12 manifest mesenteric fluid accumulation (homogeneous, clearly demarcated water density) and black arrowheads of Fig.9 and Fig.10 show engorgement of blood vessel (probably vein). Contrast enhancement of wall of distended small bowel is generally decreased, and wall of 30 of Fig.13-36 of Fig.16 seem to be well enhanced at a glance. However, high density of both wall and contents (probably bloody) by plain (nonenhanced) CT (Fig.17-Fig.20: white arrowhead) indicates hemorrhagic necrosis. In order to prove closed loop formation, start tracking down from Fig. 22. 1 obstructs at 37, and A at G of Fig.12, and there is collapsed small intestine (SB) in Fig.10 and Fig.11. Because abdominal pain increased, patient was taken to surgery where bloody ascites and hemorrhagic necrosis of small bowel were revealed. Closed loop was formed by adhesion between mesentery of small intestine, and jejunum of about 80cm length was strangulated.
|