|
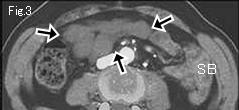
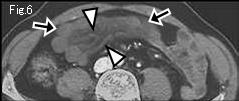
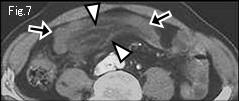
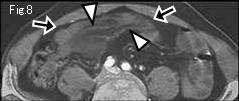
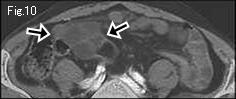
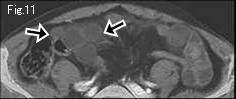
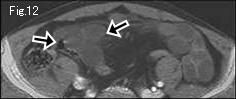
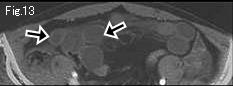
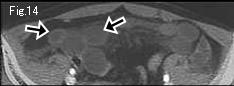
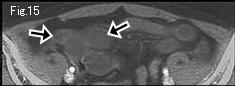
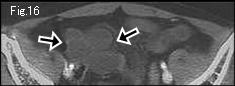
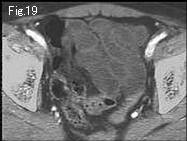
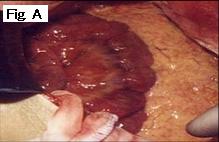
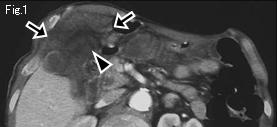
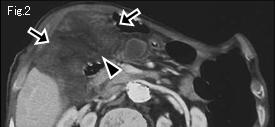
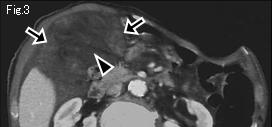
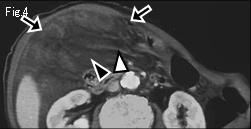
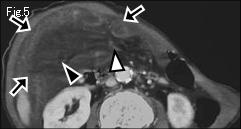
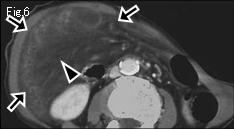
No ascites is shown in neither Fig.1 nor pelvic cavity. Because small bowel groups (black arrow of Fig.3-Fig.17) are collapsed, or only mildly dilated, it is impossible to track down them and prove closed loop formation. However, because of findings of diminished mural contrast-enhancement in comparison with uninvolved small bowel (SB), significant stranding (black arrowhead) of mesentery in Fig.4 and Fig.5, venous engorgement (white arrowhead of Fig.6-Fig.8) and gasless mildly distended small bowels, strangulated small bowel obstruction. cannot be ruled out. Based on these findings, laparotomy was performed. In central area of small intestine, 140cm length was constricted and formed closed loop by an adhesive band. Strangulated loops of bowel were congested but viable (Fig.A: intraoperative image) and no resection was needed. Strangulated obstruction without distension like this case is very rare, but should be kept in mind so as not to delay a diagnosis.
|