|
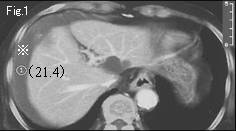
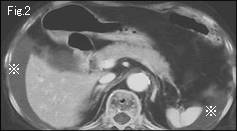
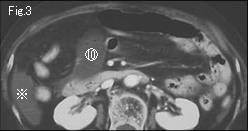
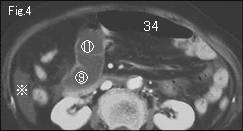
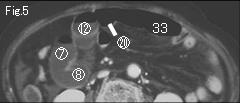
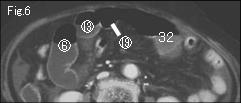
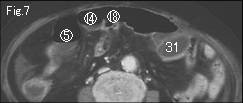
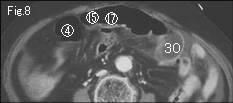
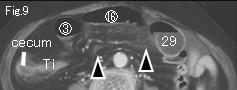
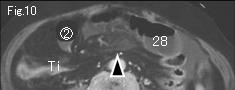
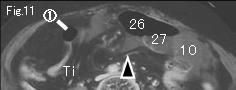
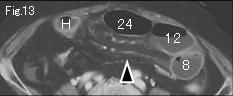
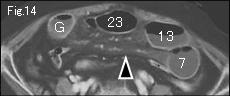
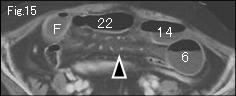
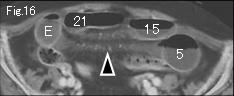
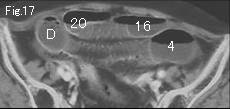
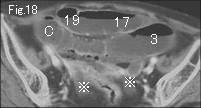
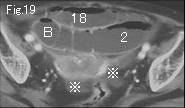
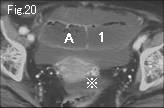
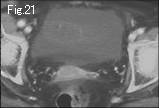
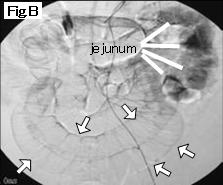
Collapsed terminal ileum (Ti) in Fig.9-Fig.12 suggests that distended small bowel indicates mechanical obstruction. Ascites (reference mark) is demonstrated in Fig.1-Fig.4 and Fig.18-Fig.20. The density(21.4HU) is measured in Fig.1, and is suggestive of diluted bloody ascites because more than 30HU is believed to indicate blood, and clear ascites between 5-15HU. Distended small bowels are not entirely gasless, besides, satisfactory mural contrast-enhancement is in favor of simple obstruction. On the other hand, quantity of ascites and significant mesenteric edema (black arrowhead) of Fig.9-Fig.16 are suggestive of strangulated obstruction. A of Fig.20 occludes at I of Fig.12 presenting beak sign (black arrow), and 1 of Fig.12 advances to 34 of Fig.4. Ti of Fig.9-Fig.12 is collapsed terminal ileum continuing to site of the obstruction (black arrow of Fig.12). Circle number 1 of Fig.11 progresses to 20 of Fig.5, and if it is considered to connect with 34 in Fig.4, then it indicates closed loop formation. However, it is impossible to track down the bowel due to gas-filled small bowels. Angiography was performed the next day because abdominal findings and pain was not alleviated. White arrowheads in Fig.A demonstrate ileocecal artery which twisted clockwise, and Fig.B depicts poor mural enhancement of ileum (white arrow) in comparison with jejunum. Diagnosis of ileal axis rotation was made and surgery was performed. 150cm ileum was necrotic (Fig.C) caused by 270 degrees clockwise torsion. In retrospective analysis, angiography or CT study after administering gastrografin from nasogastric tube or ileus tube (cf: EE Case 16) should have been performed without delay based on strangulation-suggesting findings of quantity of ascites and significant mesenteric edema, absence of whirl sign and difficulty to track down gas-filled small bowel.
|