|
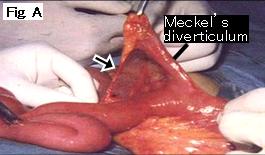
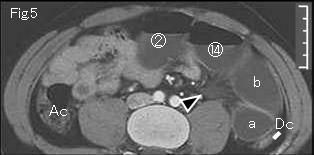
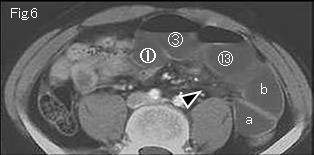
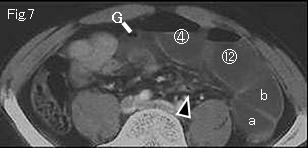
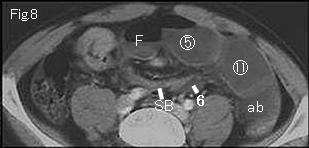
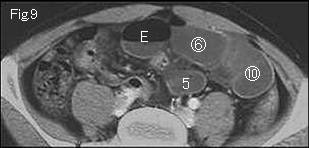
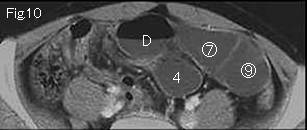
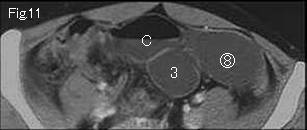
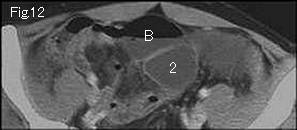
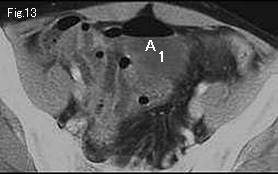
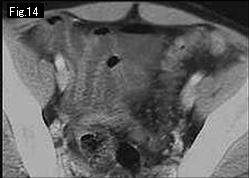
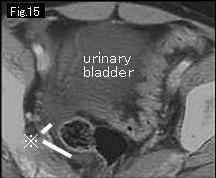
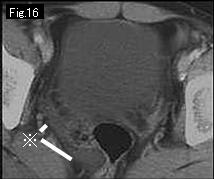
Fig.1-Fig.4 are abbreviated. Fig.5 shows no distension nor fluid content of ascending colon (Ac), and descending colon (Dc) is collapsed, accordingly distended small bowels indicate mechanical obstruction. Three findings of ascites (reference mark of Fig.15 and Fig.16 ), mesenteric stranding (Fig.5-Fig.7: black arrowhead) and distended gasless small bowels strongly suggest strangulated obstruction. On tracking down distended bowel starting from A and 1 of Fig.13, two points of obstruction are shown at 6 of Fig.8, and G of Fig.7 indicating closed loop formation. Adjacent collapsed small bowel (SB) is shown in Fig.8 and from circle number 1 of Fig.6 to circle number 14 of Fig.5 represent cephalad simple obstruction. Based on these findings, diagnosis of strangulated small bowel obstruction can be made. ab of Fig.8 are divided into a and b, and progress upward. Wall of closed loops manifests satisfactory contrast-enhancement in comparison with that of simple obstruction suggesting to be still viable. Correct CT diagnosis was made and patient was taken to emergent surgery. Meckel's diverticulum was found at 80cm from cecum (Fig.A), and mesodiverticular band (Fig.A: black arrow) adhered to mesentery forming a space, into which ileum of 25cm length was incarcerated forming closed loop. The strangulated bowel was found to be viable and no need of resection, and Meckel's diverticulum was excised.
|