|
文献考察1):特発性食道破裂の初発症状は胸痛:53%,腹痛:51%(表1).
【消化器外科領域の緊急手術・処置】 上部消化管 特発性食道破裂
Author:羽生信義(東京慈恵会医科大学 外科), 古川良幸
Source:外科(0016-593X)65巻3号 Page256-265(2003.03)
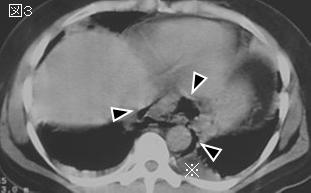
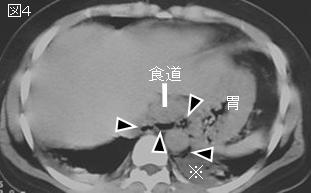
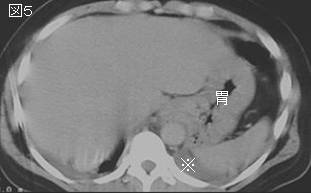
Abstract:特発性食道破裂の多くは嘔吐と関係しているために,吐物による縦隔,胸腔の汚染がひどく,早期診断が救命の鍵を握る.特発性食道破裂の消化管内容は,縦隔内を経由して椎体の両側面から流出し壁側胸膜外側の膿瘍となるので,ドレナージ術はCT,エコーを行い,的確な部位をドレナージする必要がある.基本的に,姑息的療法では治癒せしめることはできないので,外科手術療法を積極的に行い,血液浄化法,経腸栄養法,抗生物質による化学療法などの保存的治療に加えて,術中・術後にも適切なドレナージ手技が要求される.
文献考察2):Boerhaave's syndromeの要点は表2.Hamman sign(縦隔気腫の場合,心拍動に一致してバリバリという音やきしり音が聴取される)は20%に認める.
Postgrad Med J. 1997 May;73(859):265-70.
Boerhaave's syndrome.
Janjua KJ.
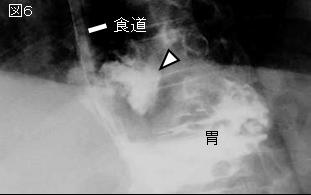
Boerhaave's syndrome or spontaneous oesophageal perforation, is a potentially lethal and frequently elusive medical condition which presents not only a diagnostic but also a therapeutic challenge. It is insufficiently considered in diagnostic hypotheses, yet may be confirmed or excluded by simple methods such as an erect chest film and a contrast study of the oesophagus. Errors in diagnosis are usually caused by unawareness of its varied and atypical presentations or failure to consider its possibility in acute cardiothoracic and upper gastrointestinal conditions. Early aggressive surgical intervention in the form of open and wide mediastinal and chest drainage, with or without oesophageal repair, resection or exclusion, offers the patient the best chance of survival against this otherwise invariably fatal event. Nonoperative therapy consisting of antibiotics, nil oral regimen, nasogastric tube suction, pleural drainage, H2 receptor blockers and either a feeding enterostomy or total parenteral nutrition, may also be appropriate in selected patients. It is probable that the condition is more common than is generally supposed. All clinicians need to be aware of this lethal disease, its frequently unusual presentations and the importance of early diagnosis.PMID: 9196697
|







;){kind=link}
;){kind=link}