|
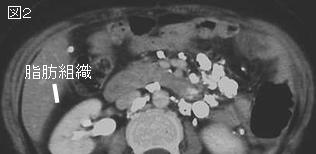
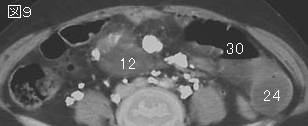
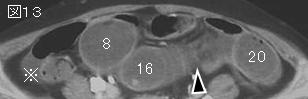
partial volume effect(部分容積効果):あるCT値を持った物体がスライスの一部にしか含まれないとすると,その周囲の構造のCT値と平均化され,物体は真のCT値よりも高いあるいは低いCT値を持つ構造として表現され,辺縁がぼやける.これをpartial volume effectと言い,上図の右2つにpartial volume effectが発生する.
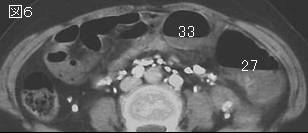
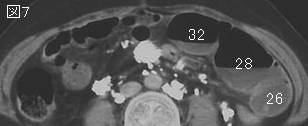
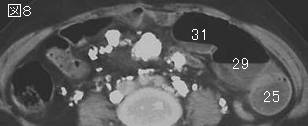
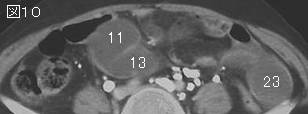
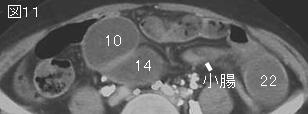
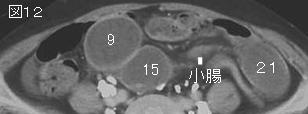
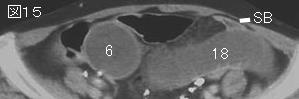
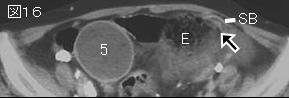
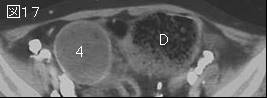
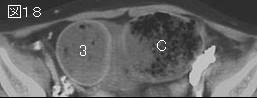
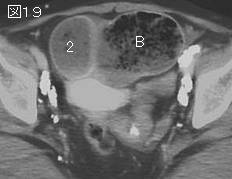
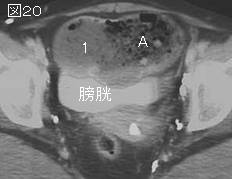
文献考察:小腸内糞便(small bowel feces ).小腸閉塞例の55.9%に認められ,閉塞部位または閉塞部位近辺を意味する場合が多い.
AJR Am J Roentgenol. 2004 Nov;183(5):1361-6.
Frequency and relevance of the "small-bowel feces" sign on CT in patients with small-bowel obstruction.
Lazarus DE, Slywotsky C, Bennett GL, Megibow AJ, Macari M.
OBJECTIVE: We sought to determine the incidence of the "small-bowel feces" sign (SBFS) in patients with small-bowel obstruction (SBO) and whether it can be used to accurately locate the point of obstruction. SUBJECTS AND METHODS: From November 2002 until March 2003, 34 consecutive adult patients with CT findings of small-bowel obstruction were prospectively evaluated. The CT findings used to diagnose small-bowel obstruction were a dilated proximal small bowel and a collapsed distal small bowel and colon. CT scans were evaluated to determine the degree of obstruction (mild, moderate, or high-grade), the presence or absence of the SBFS (defined as particulate-type material in the dilated small bowel), the location of the SBFS in relation to the transition zone, and the cause of the obstruction. Mild obstruction was defined as a slight discrepancy between the caliber of the proximal and that of the distal small bowel; moderate SBO was defined as a discrepancy of 50% or more between the calibers of the proximal and the distal small bowel; and high-grade SBO was considered to be present if the distal small bowel and the colon had collapsed. The cause of the obstruction was determined from surgical findings or a combination of CT findings, follow-up barium studies, and clinical assessment. RESULTS: The SBFS was present in 19 (55.9%) of 34 patients with SBO. The degree of SBO was mild in six, moderate in 11, and high-grade in 17 of the patients. The SBFS was present in one of the six patients (16.6%) with mild, eight (72.7%) of the 11 with moderate, and 10 (58.8%) of the 17 with high-grade SBO. In all patients in whom the SBFS was present, the particulate material could be traced to the point of transition and was most conspicuous in the transition zone. The length of fecallike material ranged from 2 to 25 cm and was longer in moderate and high-grade SBO than in mild SBO. The cause of the SBO was an adhesion in 20 patients, a hernia in four patients, Crohn's disease in four patients, a tumor in three patients, and other miscellaneous causes in three patients. CONCLUSION: When present on CT, the SBFS can be used to help locate the transition zone in patients with SBO. The sign is present more frequently in patients with moderate and high degrees of SBO.PMID: 15505304
|




;){kind=link}