|
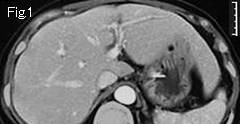
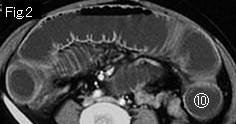
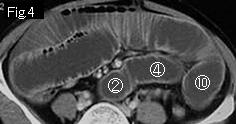
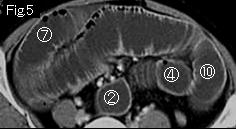
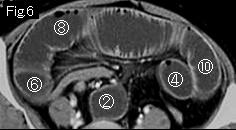
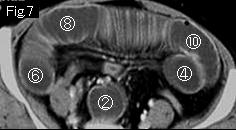
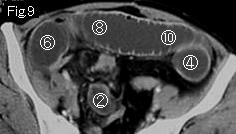
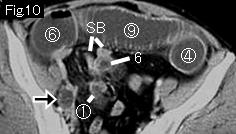
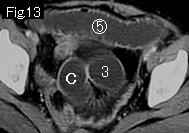
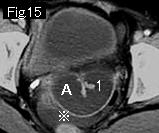
Distension limited to small bowel indicates small bowel obstruction. There is no ascites in the epigastrium (Fig.1), but a small quantity in pelvic cavity (Fig.14 and Fig.15: reference mark). The small bowel which is dilated more than 2.5cm outside diameter shows contrast-enhanced viable wall. Gasless distension of small bowel, ascites and mesenteric edema (Fig.12: black arrowhead) suggest strangulated obstruction. Start tracking down from A1 of Fig.15 to search whether it forms closed loop. 2 of Fig.14 connects to obstruction site (6 of Fig.10), and B of Fig.14 obstructs at E of Fig.11, and there is collapsed small bowel (SB) in Fig.10 and Fig.11, demonstrating closed loop. The circle number 1 of Fig.10 where simple obstruction starts and move on to circle number 10 of Fig.2. Consequently, the diagnosis as strangulated small bowel obstruction of about 15cm length without necrosis can be made. Black arrow of Fig.10-Fig.12 is an ovarian cyst. When strangulated bowel obstruction occurs after gynecologic surgery, sigmoidectomy and appendectomy, strangulated bowel is located in a pelvic cavity in most cases. Surgery revealed strangulated, but viable small bowel obstruction of 15cm ileum by an adhesive band, severance of a band was all required.
|