|
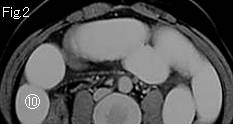
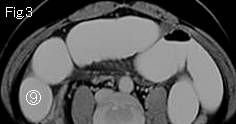
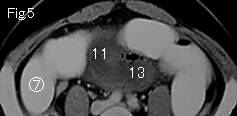
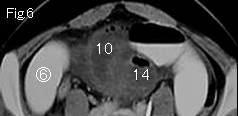
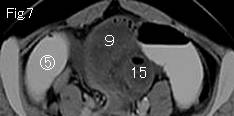
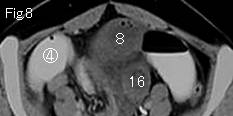
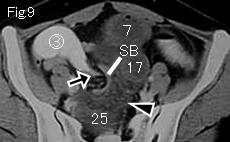
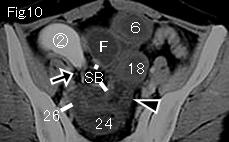
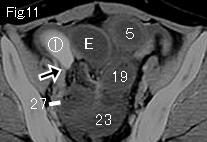
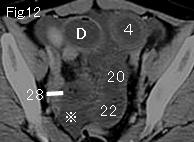
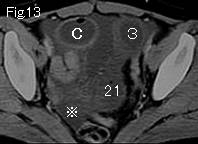
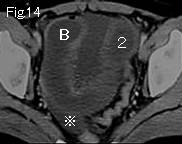
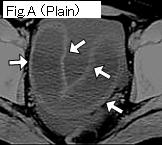
The collapsed colons in Fig.4 and dilated small bowel indicate small bowel obstruction. In most cases for paralytic ileus, right colon contains fluid with/or without gas similarly to small bowel. There is massive ascites around the liver(Fig.1: reference mark), and a little in pelvic cavity (Fig.12-Fig.15: reference mark). The dilated small bowel which does not contain gastrografin is gasless (no gas or little gas), and there is mesenteric fat stranding (Fig.9 and Fig.10: black arrowhead). These 3 findings of ascites, dilated gasless small bowel and mesenteric fat stranding suggest high possibility of strangulated small bowel obstruction. Evidence of closed loop formation results in definite diagnosis of strangulated small bowel obstruction and can be proved by tracking down the distended small bowel. Starting from 1 of Fig.15, it arrives at obstruction site of 28 of Fig.12. A of Fig.15 at another obstruction site F of Fig.10, and there are collapsed small bowels (SB) in Fig.9 and Fig.10. Black arrows of Fig.9-Fig.11 show "bird's beak sign" indicating simple obstruction site, and move on to caudal side from circle number 1 to circle number 10 of Fig.2. Wall of U-shaped small intestine of Fig.14 and Fig.15 seems to be contrast-enhanced at a glance, however, noncontrast CT of Fig.A (white arrow) presents high density indicating hemorrhagic necrosis (Fig.B). In cases that strangulated bowel obstruction is suspected, but it is difficult to prove closed loop, CT study after administering gastrografin from nasogastric tube or ileus tube is an extremely useful examination.
|