|
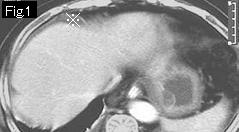
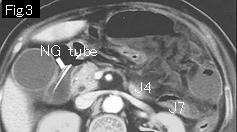
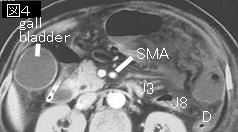
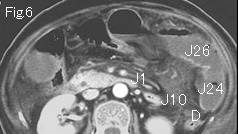
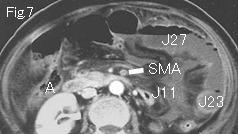
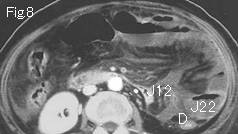
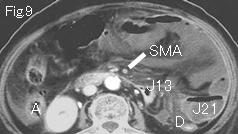
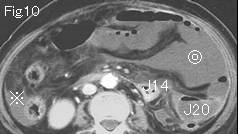
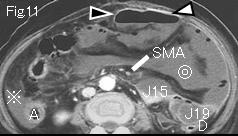
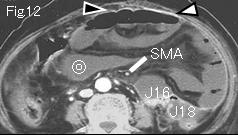
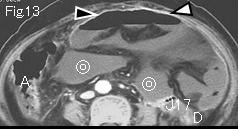
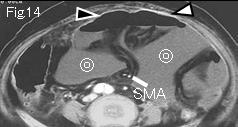
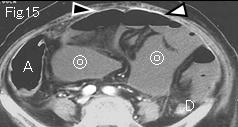
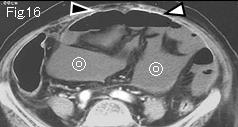
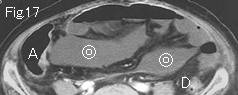
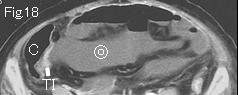
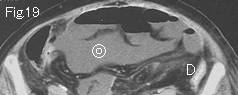
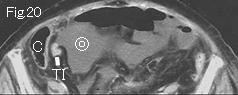
There is ascitic fluid (reference mark) around liver of Fig.1 as well as in the right paracolic gutter of Fig.10 and Fig.11. It is essential to check out whether SMA (superior mesenteric artery) is occluded by embolus if the patient with atrial fibrillation presents with abdominal pain. SMA starts at Fig.2 and distal SMA from Fig.7 is not contrast-enhanced indicating SMA occlusion by embolus. Seemingly ascites-looking double circle from Fig.10 is not ascites, but it is actually necrotic small bowel without blood supply. As for the terminal ileum (TI), the right colon (A: ascending colon, C: cecum) and the descending colon (D), their wall is normally contrast-enhanced .On tracking down Jejunal (J1) beginning in Fig.6, it makes U-turn in Fig.2, and then descends, and makes another U-turn in Fig.13 again, and contrast enhancement of wall disappears from jejunum (J27) of Fig.7. Black arrowhead and white arrowhead of Fig.11-Fig.16 appear to be small intestinal wall strongly contrast-enhanced at a glance, but, in fact, white arrowhead is peritoneum, and black arrowhead is mesentery which are thickened because they are in direct contact with advanced necrosis of bowel wall extending to serosa. Note posterior wall is not contrast-enhanced at all. It is one of pitfalls on diagnosis of bowel necrosis, as well as high density with the hemorrhagic necrosis that seems to be contrast-enhanced. The more peripheral SMA from Fig.12 is contrast-enhanced due to blood supply from collateral vessels. This finding suggest collateral pathway which developed after necrosis, or blood supply not enough to prevent necrosis. Surgery 2 days later revealed massive necrosis of small bowel and right colon.
|