|
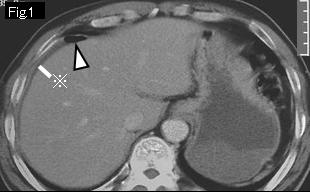
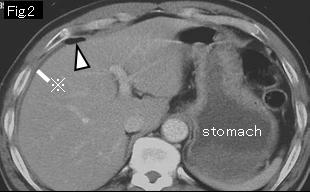
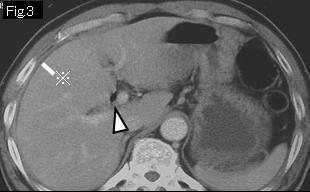
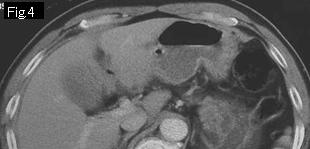
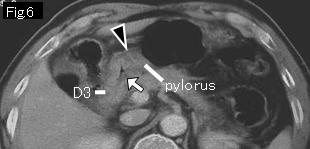
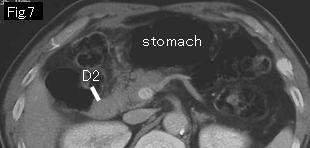
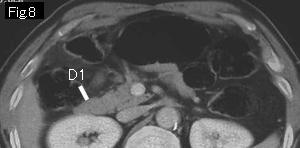
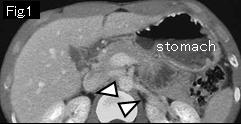
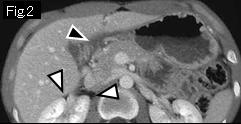
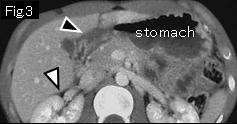
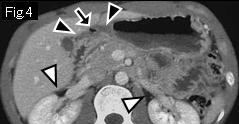
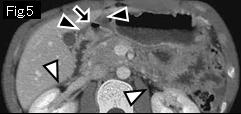
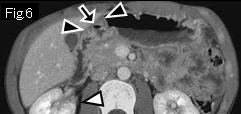
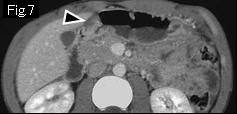
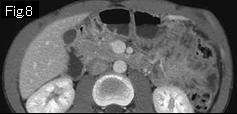
There are free air (white arrowhead) and a little ascites (reference mark) in Fig.1-Fig.3. Because no submucosal edema is identified in gastric wall, there seems to be no acute lesion in stomach. Tracking up duodenum from D1 of Fig.8 to cephalad side, it becomes duodenal bulb at D3 of Fig.6. Anterior wall of duodenal bulb presents edematous wall thickening (Fig.5 and Fig.6: black arrowhead). The white arrow indicates duodenal lumen, and black arrow of Fig.5(gas in edematous wall) should be taken to be a wall defect, namely a duodenal ulcer, which leads to a diagnosis of the perforated duodenal ulcer. Because abdominal finding revealed board-like rigidity confined to only epigastrium and ascites is of minimal amount, conservative treatment was chosen with success. Endoscopy 12 days later showed an ulcer of anterior wall of duodenal bulb.
|