|
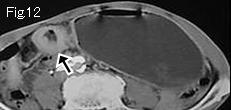
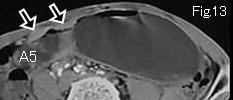
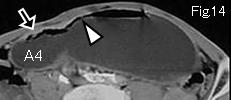
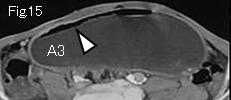
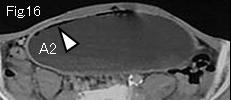
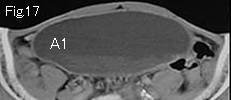
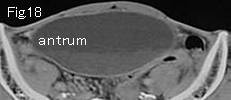
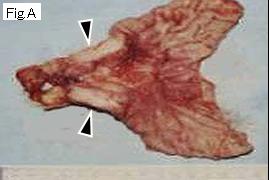
There is no free air or ascites. Stomach is distended remarkably so as to reach pelvic cavity. Start tracking down from antrum A1 of Fig.17 to caudal side to search for any lesions causing obstruction. Wall thickening (black arrows) begins in Fig.14, and it ends up to circumferential lesion of Fig.12 and Fig.11, which indicate neoplasmic lesion causing complete occlusion in Fig.10 (black arrow). It is localized, strongly and irregularly contrast-enhanced, suggesting a malignant lesion. Because the gas (white arrowhead) right under anterior wall of stomach of Fig.14-Fig.16 does not form air-fluid level (niveau), it should be considered as intramural gas (pneumatosis intestinalis). Regardless of kind of a lesion, when there are mucosal disruption and increased intraluminal pressure, intramural gas can be produced, it does not necessarily indicate ischemia or necrosis of wall. Fig.A is resected specimen, and black arrowheads represent gastric cancer. Pathology reported as poorly differentiated adenocarcinoma.
|