|
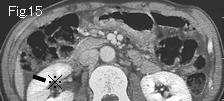
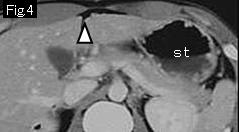
Reference Case (perforated duodenal ulcer): A 17-year-old male presented with acute onset of epigastric pain and vomiting for 12 hours. Body temperature:37.0 degrees Celsius. On examination, there were tenderness and rebound tenderness with muscle guarding in right upper quadrant.
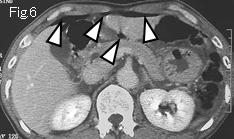
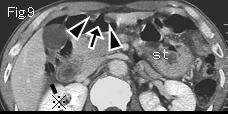
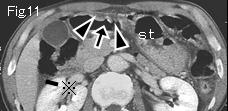
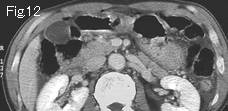
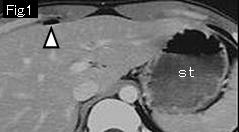
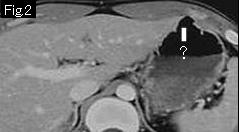
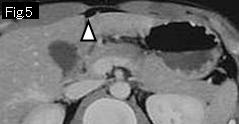
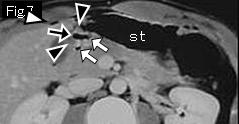
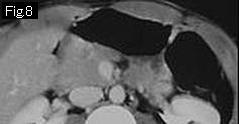
White arrowheads of Fig.1 and Fig.3-Fig.7 present free air. The lesser curvature and antrum of stomach do not demonstrate edematous wall thickening, or an acute ulcerative lesion. Fig.6 and Fig.7 show the gastroduodenal junction (pylorus). Anterior wall of duodenal bulb is edematous and thickened (black arrowhead). White arrowheads are extraluminal free air, whereas white arrows are intraluminal gas, and black arrows are gas in duodenal ulcer. As a result, the diagnosis of perforated duodenal ulcer can be made. "?" of Fig.2 and Fig.3 is not an acute ulcerative lesion because it is not accompanied by edematous thickening of surrounding wall .st: stomach. Laparotomy revealed perforation (5mm in size) in anterior wall of duodenal bulb.
|








;){kind=link}