|
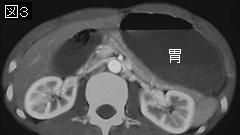
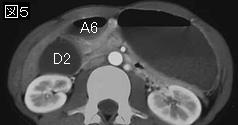
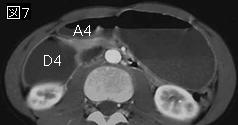
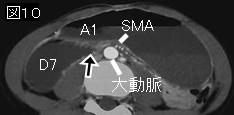
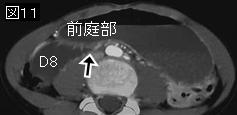
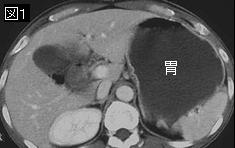
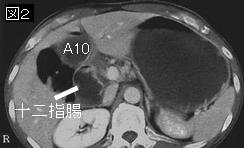
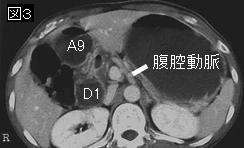
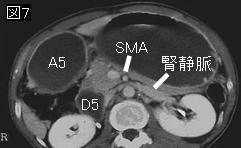
文献考察1):SMA syndrome.CTとUS検査による診断基準は,十二指腸がSMA背側を通過する部位でSMA-Aorta distance:8mm以下,SMA-Aorta angle:22度以下.
Diagn Interv Radiol. 2005 Jun;11(2):90-5.
Superior mesenteric artery syndrome: CT and ultrasonography findings.
Unal B, Aktas A, Kemal G, Bilgili Y, Guliter S, Daphan C, Aydinuraz K.
PURPOSE: The purpose of the study was to describe computed tomography (CT) and ultrasonography findings in superior mesenteric artery syndrome (SMAS). MATERIALS AND METHODS: The study was performed on 89 CT examinations. Ultrasonography was performed on 32 and barium study was performed on four of these subjects. Group A consisted of cases with one or more of the following complaints: postprandial epigastric pain, weight loss and vomiting. Group B consisted of the remaining cases. Cases who had all of the above-mentioned clinical findings and duodenal dilatation, to-and-fro barium movement and SMA indentation in barium study were diagnosed as having SMAS. Body mass index (BMI, kg/m2) was calculated. The distance between SMA and aorta, at the location where the duodenum passes from, was measured on CT and ultrasonography. The angle between SMA and aorta was measured on ultrasonography images. Group and gender differences were analyzed with t-test, the relationship between clinical and CT findings was analyzed with Mann Whitney U test and the relations between BMI-CT and CT-ultrasonography measurements were analyzed with Pearson coefficients. RESULTS: Of 13 cases in Group A, 3 were diagnosed as SMAS. Eight of the cases showed gastric and/or duodenal dilatation. In 6 cases, antrum had an abnormally high location at portal hilus. In Group A, the SMA-aorta distance was 6.6 +/- 1.5 mm and the SMA-aorta angle was 18.7 +/- 10.7 degrees . In Group B, these values were 16.0 +/- 5.6 mm and 50.9 +/- 25.4 degrees , respectively (p
文献考察2):腎静脈捕捉症候群(nutcracker syndrome,nutcracker phenomenon).
Eur Radiol. 2005 Aug;15(8):1745-51.
Nutcracker or left renal vein compression phenomenon: multidetector computed tomography findings and clinical significance.
Cuellar i Calabria H, Quiroga Gomez S, Sebastia Cerqueda C, Boye de la Presa R, Miranda A, Alvarez-Castells A.
The use of multidetector computed tomography (MDCT) in routine abdominal explorations has increased the detection of the nutcracker phenomenon, defined as left renal vein (LRV) compression by adjacent anatomic structures. The embryology and anatomy of the nutcracker phenomenon are relevant as a background for the nutcracker syndrome, a rare cause of hematuria as well as other symptoms. MDCT examples of collateral renal vein circulation (gonadal, ureteric, azygous, lumbar, capsular) and aortomesenteric (anterior) and retroaortic (posterior) nutcracker phenomena in patients with no urologic complaint are shown as well as studies performed on patients with gross hematuria of uncertain origin. Incidental observation of collateral veins draining the LRV in abdominal MDCT explorations of asymptomatic patients may be a sign of a compensating nutcracker phenomenon. Imbalance between LRV compression and development of collateral circulation may lead to symptomatic nutcracker syndrome.PMID: 15742169
要旨:左腎静脈の長さは約7.5cmで,右側の3倍長い.合流する静脈は,右側は尿管静脈だけであるのに対し,左側はgonadal vein(精巣静脈,卵巣静脈),尿管静脈,下横隔膜静脈と副腎静脈である.両側とも後腹膜の静脈と豊富なnetworkを有する.さらに左側は奇静脈系や脾静脈(70%)と連続する場合も多い.腎静脈捕捉症候群(nutcracker syndrome,nutcracker phenomenon)は左腎静脈が血管に圧迫され腎静脈圧が亢進した状態で,anterior nutcracker phenomenon(大動脈とSMA間)とposterior nutcracker phenomenon(retroaortic renal vein→大動脈と脊椎間:下記2例目の参照症例)がある.側副路が豊富なため大部分は無症候であるが,まれに血尿,たんぱく尿や腰痛の原因となることがある.
|