|
文献考察1):魚骨の腸管穿破による肝膿瘍,集計12例(表1,2)
Surg Today. 1999;29(9):922-6.
Successful treatment of a hepatic abscess that formed secondary to fish bone penetration by percutaneous transhepatic removal of the foreign body: report of a case.
Horii K, Yamazaki O, Matsuyama M, Higaki I, Kawai S, Sakaue Y.
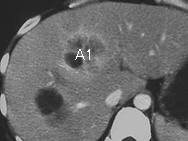
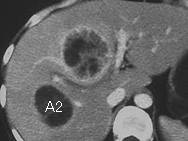
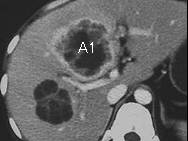
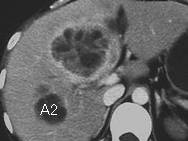
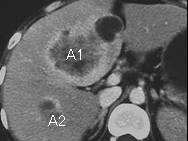
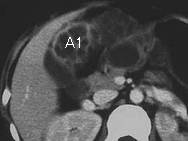
We describe herein the case of a hepatic abscess that developed secondary to fish bone penetration which was successfully treated without laparotomy. A 61-year-old man was admitted to our hospital with a high fever that had persisted for 2 weeks in spite of medication. Abdominal ultrasonography (AUS) and computed tomography (CT) of the abdomen revealed a hepatic abscess with a linear calcified foreign body and gas. Percutaneous abscess drainage was performed under ultrasonographic guidance. After drainage, the patient became afebrile, and AUS and CT findings demonstrated that the abscess cavity had decreased in size, but still contained the foreign body. Under ultrasonographic guidance and fluoroscopy, we inserted endoscopic forceps into the sinus tract and succeeded in removing the foreign body from the liver. It was found to be a fish bone that was 2.8 cm long and 0.3 cm wide.PMID: 10489138
文献考察2):異物の腸管穿破による肝膿瘍,集計20例(表3)
BMC Surg. 2003 Oct 7;3:8.
Liver abscess secondary to a broken needle migration--a case report.
Chintamani, Singhal V, Lubhana P, Durkhere R, Bhandari S.
BACKGROUND: Perforation of gut by sharp metallic objects is rare and rarer still is their migration to sites like liver. The symptoms may be non-specific and the discovery of foreign body may come as a radiological surprise to the unsuspecting clinician since the history of ingestion is difficult to obtain. CASE REPORT: A unique case of a broken sewing needle in the liver causing a hepatic abscess and detected as a radiological surprise is presented. The patient had received off and on treatment for pyrexia for the past one year at a remote primary health center. Exploratory laparotomy along with drainage of abscess and retrieval of foreign body relieved the patient of his symptoms and nearly one-year follow up reveals a satisfactory recovery. CONCLUSION: It is very rare for an ingested foreign body to lodge in the liver and present as a liver abscess. An ultrasound and a high clinical suspicion index is the only way to diagnose these unusual presentations of migrating foreign bodies. The management is retrieval of the foreign body either by open surgery or by percutaneous transhepatic approach but since adequate drainage of the abscess and ruling out of a fistulous communication between the gut and the liver is mandatory, open surgery is preferred.PMID: 14531934(full text)
文献考察3):肝放線菌症
感染症症候群 細菌感染症 肝・胆道感染症 肝放線菌症
Author:伊藤章(横浜市立大学医学部附属病院 臨検査)
Source:日本臨床(0047-1852)別冊感染症症候群I Page449-450(1999.01)
要旨:放線菌症は, 嫌気性あるいは通性嫌気性で非抗酸性の無胞子グラム陽性桿菌で,健康人の口腔から高率に検出される常在細菌Actinomyces israeliiその他の放線菌属によって引き起こされる慢性の化膿性および肉芽腫性疾患である. 病巣の中に膿瘍が形成され, 瘻孔を生じ排出される膿中に菌を含む硫黄顆粒(sulfur granule)をみる.病巣部位により頚顔部, 胸部, 腹部,その他の放線菌症にわけられる.頻度は頚顔部が半数以上, 胸部約15%,腹部(回盲部に多い)約20%,その他少数である.肝放線菌症は通常は腹部放線菌症あるいは胸部放線菌症から2次的に生じるが, まれに原発性放線菌症があり,腫瘤を形成し癌と間違えられたり, ときに肝膿瘍や横隔膜膿瘍を起こす.
文献考察4):肝放線菌症,本邦集計22例(表4,5)
肝放線菌症の1切除例
Author:大司俊郎(友愛記念病院 外科), 加藤奨一, 加藤修志, 兼信正明, 山本修, 鹿野信吾
Source:臨床外科(0386-9857)59巻2号 Page243-247(2004.02)
Abstract:72歳男.上腹部痛を主訴とした.画像検査で肝内胆管癌を疑い肝生検を施行したところ,好中球,リンパ球,形質細胞等の炎症細胞浸潤と線維化が認められたのみであった.炎症性腫瘤等も考えられたが,画像診断などから悪性腫瘍を否定できず,腹痛,発熱等の原因も肝腫瘤に原因があると考えられたことから切除術を施行した.術中所見より外側区域肝内胆管癌の肝円索及び胃浸潤と判断し,幽門側胃合併切除を伴う肝左葉切除,リンパ節郭清,Billroth II法再建術を施行した.病理学的所見では,肉芽腫性・膿瘍性の変化で内部に放線菌症に特異的な菌塊を認め,門脈領域にも病変は波及していた.第17病日に発熱を伴う左足部関節痛が出現し,MRIで左足部関節炎と診断した.放線菌による関節炎も考慮し,アンピシリンとミノサイクリンの投与を行い,徐々に症状は改善した.
|












;){kind=link}
;){kind=link}
;){kind=link}
;){kind=link}
;){kind=link}