|
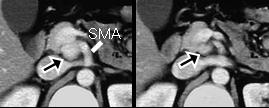
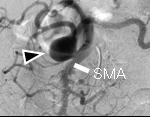
文献考察1):肝動脈瘤.全腹部内臓動脈瘤306例中肝動脈瘤は36例(12%).有症状のもの,多発性と非動脈硬化例(fibromuscular dysplasia, polyarteritis nodosa, history of endocarditis)が破裂しやすい因子でinterventionの適応である.
J Vasc Surg. 2003 Jul;38(1):41-5.
Hepatic artery aneurysm: factors that predict complications.
Abbas MA, Fowl RJ, Stone WM, Panneton JM, Oldenburg WA, Bower TC, Cherry KJ, Gloviczki P.
OBJECTIVE: We reviewed the Mayo Clinic experience with management and outcome of hepatic artery aneurysms (HAA). METHODS: Retrospective review of charts for 306 patients with true visceral aneurysm diagnosed from 1980 to 1998 enabled identification of 36 patients (12%) with HAA. RESULTS: Patients with HAA included 23 men and 13 women, with mean age of 62.2 years (range, 20-85 years). Most aneurysms were extrahepatic (78%) and single (92%). Mean aneurysm diameter at presentation was 3.6 cm (range, 1.5-14 cm). Five aneurysms had ruptured (14%), and four were symptomatic (11%). Mortality from rupture was 40%. Of the 9 patients with ruptured or symptomatic aneurysms, 2 patients had multiple HAA, 3 patients had fibromuscular dysplasia, and 2 patients had polyarteritis nodosa. All five HAAs that ruptured were of nonatherosclerotic origin (P =.001). Fourteen patients (39%) underwent elective procedures, including excision with vein graft (n = 7), excision with dacron graft (n = 3), excision alone (n = 2), and percutaneous embolization (n = 2). Two vein grafts and one dacron graft became occluded within 1 year. Nonoperative management was elected in 22 patients (61%) with mean aneurysm diameter 2.3 cm (range, 1.5-5 cm). No complications related to the aneurysm occurred during mean follow-up of 68.4 months (range, 1-372 months). Aneurysm growth was identified in 27%, the greatest being 0.8 cm over 34 months. CONCLUSIONS: HAA are at definite risk for rupture (14%). Risk factors for rupture include multiple HAA and nonatherosclerotic origin. Patients with symptomatic aneurysms or any of these risk factors should be considered for intervention.PMID: 12844087
本文中のCONCLUSIONS:Although rare, HAA are at definite risk for rupture. Not all HAA need intervention, and small (
文献考察2):腹部内臓動脈瘤破裂.死亡率は25%.腹腔動脈瘤破裂の死亡率は100%に近い.
J Vasc Surg. 2001 Apr;33(4):806-11.
Visceral artery aneurysm rupture.
Carr SC, Mahvi DM, Hoch JR, Archer CW, Turnipseed WD.
PURPOSE: Aneurysms of the visceral arteries are infrequently encountered. Many are found incidentally and are thought to have a benign outcome. To better characterize these lesions and their clinical course, we reviewed our experience with visceral artery aneurysms (VAAs) at a single institution. METHODS: A retrospective analysis of all VAAs diagnosed at our institution over the past 10 years was performed. The presentation, management, and outcome of therapy was examined for each patient. RESULTS: Thirty-four VAAs in 26 patients were diagnosed over the past 10 years. Four patients had multiple VAAs: splenic (17), hepatic (7), celiac (3), superior mesenteric (2), gastroduodenal (2), pancreaticoduodenal (1), right gastric (1), ileal (1) artery aneurysms. Associated aneurysms were found in 31% of patients and involved the thoracic aorta (3 patients), abdominal aorta (4 patients), renal arteries (2 patients), iliac artery (3 patients), lower extremity (1 patient), and intracranium (1 patient). In 15 patients (58%), VAAs were detected before rupture by chance or because abdominal symptoms resulted in diagnostic evaluation. Eight of these underwent elective surgery, and there were no deaths. Of those 15 patients with known VAAs, one patient died of rupture and hemorrhage from an untreated splenic artery aneurysm. Eleven patients (42%) presented unexpectedly with rupture, and two died despite prompt surgical treatment. The mortality rate in patients who had ruptured VAAs was 25%, including those who presented with ruptured aneurysms and those observed whose aneurysms eventually ruptured. CONCLUSIONS: Aneurysms of the visceral arteries are rare but important vascular lesions. Associated aneurysms are common. Because of the risk of rupture, often with a fatal outcome, an aggressive approach to the treatment of VAA is essential.PMID: 11296336
|