|
文献考察1):肝血管腫本邦集計87例.
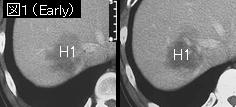
尾状葉原発と考えられた肝巨大血管腫の1切除例 本邦報告例の検討
Author:森景則保(山口大学 第1外科), 守田信義, 江里健輔, 他
Source:消化器外科(0387-2645)19巻9号 Page1499-1504(1996.08)
要旨:腫瘍最大径4cm以上のものは腹部症状(腹満感・腹痛)を訴える例が多く巨大血管腫と定義されている.重篤な合併症に腫瘍破裂とKasabach-Merritt症候群がある.Kasabach-Merritt症候群の発症機序は,血管腫内の拡張した異常血管内面において血液のうっ滞と凝固系の活性化が起こり,フィブリン網および血栓が形成されることにより凝固因子の消耗による出血傾向と二次性線溶系亢進が生じる.手術適応は,4cm以上で,1)増大傾向,2)凝固線溶系異常,血小板減少あるいはmicroangiopathic hemolytic anemia,3)持続する腹部症状,4)肝表面で腫瘤触知,などのいずれかを認める場合.
文献考察2):肝血管腫のmanagement
J Am Coll Surg. 2003 Sep;197(3):392-402.
Diagnosis, management, and outcomes of 115 patients with hepatic hemangioma.
Yoon SS, Charny CK, Fong Y, Jarnagin WR, Schwartz LH, Blumgart LH, DeMatteo RP.
BACKGROUND: Hepatic hemangiomas are congenital vascular malformations and are the most common benign hepatic tumors. Because the use of cross-sectional imaging has increased, benign hepatic tumors, especially hemangiomas, are encountered more frequently, so clinicians should be familiar with the most appropriate diagnostic tests, management, and outcomes of patients with hepatic hemangioma. STUDY DESIGN: All patients with a primary diagnosis of hepatic hemangioma referred for surgical evaluation at our institution between January 1992 and December 2000 were identified from a prospective database. Demographics, presentation, tumor characteristics, diagnostic studies, surgical procedures, and outcomes were analyzed. RESULTS; Of 115 patients in the study, nearly half were asymptomatic. In symptomatic patients, abdominal pain or discomfort was the most common presenting symptom. At our institution, the diagnosis of hemangioma was established by ultrasonographic studies in 57% of patients tested, by CT scan in 73%, and by MRI in 84%. In patients with large tumors considered for resection, direct angiography or, more recently, CT angiography, confirmed the diagnosis in 27 of 29 patients (93%). Enucleation was performed in 31 (60%) of the 52 patients who underwent surgical resection; 63 patients were observed. Postoperative complications occurred in 13 patients (25%), and there were no perioperative deaths. Of the patients with symptoms before resection, 96% had resolution of symptoms after operation. CONCLUSIONS: Hepatic hemangioma can be diagnosed in most patients using noninvasive studies, particularly MRI. Hepatic hemangiomas can be removed safely if patients become symptomatic or when malignancy cannot be excluded. CT angiography can be a valuable preoperative study in patients with large tumors, and enucleation is the procedure of choice. In asymptomatic or minimally symptomatic patients, hepatic hemangiomas usually have a benign course and can be observed.PMID: 12946794
追記:52例の手術適応は,有症状(60%),悪性を否定できない(29%)と増大(11%)であった.症状が軽いまたはない例は経過観察でいい.
文献考察3):1-4%が自然破裂を起こし,30例の報告例の死亡率は60%.10cm以上で有症状であれば手術の適応.
Ann Ital Chir. 2000 May-Jun;71(3):379-83.
Spontaneous rupture of a giant hemangioma of the liver.
Cappellani A, Zanghi A, Di Vita M, Zanghi G, Tomarchio G, Petrillo G.
Hemangiomas are frequent benign tumors of the liver. Symptoms (abdominal pain and fullness) are mostly seen in giant lesions. Rupture is the most severe complication, can occur spontaneously, with intraperitoneal bleeding, in 1-4% of hemangiomas and has been described in about 30 cases in the international literature with a high mortality (about 60%). This complication is the principal indication for surgery. Although spiral CAT scan and MR are actually the most efficacious imaging methods for study of liver hemangiomas, after Echography, emergency techniques that allows a simultaneous therapeutic approach--as is angiography--are preferable. Trans-arterial embolization (TAE) is in fact useful to stop bleeding and then to perform a safer surgery. A successful embolization can delay the surgical resection of the hemangioma for the time necessary to recover from the hemodynamic distress. Aside from the success of angiographic approach, surgery remains mandatory, effective in stopping the bleeding and in preventing re-bleeding or other complications of TAE such as abscess, fever, etc.. Intraoperative echography currently is the best method to identify vasculo- biliary anatomy and to perform a correct resection. The absence of risk factors for spontaneous rupture of liver hemangiomas, makes this event unpredictable. The best treatment for non-ruptured hemangiomas is still controversial but surgery is usually limited to symptomatic tumors larger than 10 cm.PMID: 11014019
文献考察4):自然破裂の死亡率は36.4%.
Surg Today. 2003;33(6):459-63.
Hemoperitoneum from a spontaneous rupture of a giant hemangioma of the liver: report of a case.
Corigliano N, Mercantini P, Amodio PM, Balducci G, Caterino S, Ramacciato G, Ziparo V.
Hemangioma is the most common benign tumor of the liver and it is often asymptomatic. Spontaneous or traumatic rupture, intratumoral bleeding, consumption coagulopathy, and rapid growth are mandatory surgical indications. We report a case of giant hemangioma of hepatic segments II and III, which presented as hemoperitoneum, and were treated successfully with preoperative transcatheter arterial embolization (TAE) and hepatic bisegmentectomy. A PubMed Medline search has identified up to now 32 cases of spontaneous rupture of hepatic hemangioma in adults (age >14 years) without a history of trauma, including the present case. Twenty-seven out of these were reviewed. Sixteen (84.2%) of 19 tumors of known size were giant hemangiomas (mean diameter 14.8 cm; range 6-25). Twenty-two (95.7%) patients underwent surgery. Thirteen patients (59.1%) had a resection, 5 (22.8%) were sutured, and 4 (18.1%) underwent tamponade. Three (23%) out of the 13 resected patients died. Four patients (30.8%) underwent TAE prior to elective hepatic resection without any operative mortality. Among the 5 sutured patients, 2 (40%) died as well as 3 (75%) out of 4 patients who underwent tamponade. The mortality rate of all surgery patients was 36.4% (8/22).PMID: 12768374
|