|
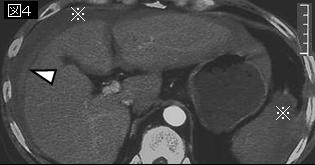
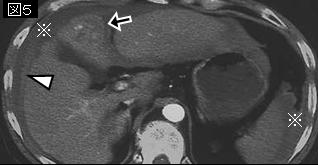
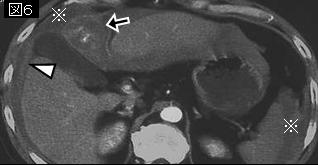
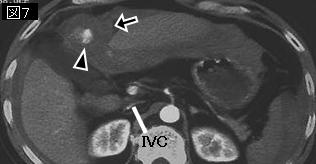
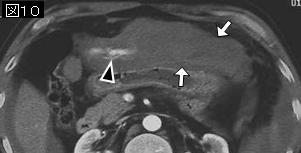
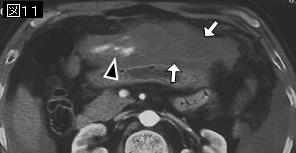
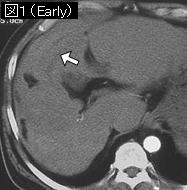
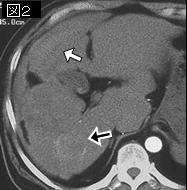
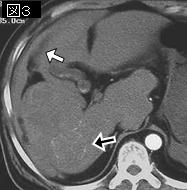
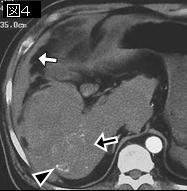
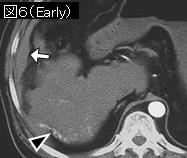
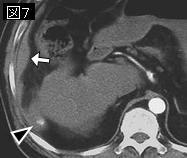
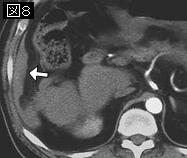
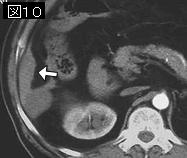
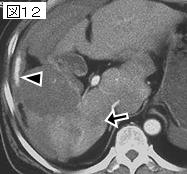
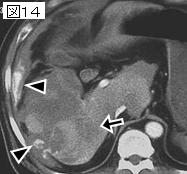
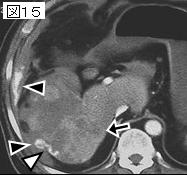
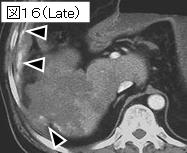
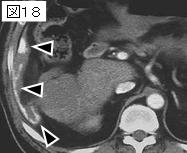
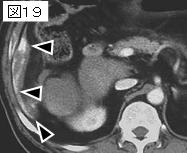
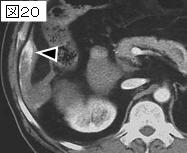
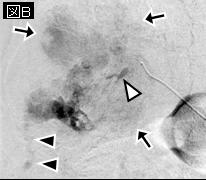
文献考察1):肝細胞癌破裂のCT所見:肝表面近くに存在する腫瘍,肝表面から突出する腫瘍,肝表面の断裂像(discontinuity)と周辺の血腫.
Br J Radiol. 2001 Feb;74(878):142-6.
The findings of ruptured hepatocellular carcinoma on helical CT.
Choi BG, Park SH, Byun JY, Jung SE, Choi KH, Han JY.
To evaluate the helical CT findings of ruptured hepatocellular carcinoma (HCC), 12 patients with ruptured HCC were reviewed with regard to the tumour's location, size and contour protrusion, the appearance of the mass, the enhancement pattern, multiplicity and secondary changes. All ruptured tumours were located at the periphery of the liver and had a protruding contour. The maximum diameter of tumours ranged from 2 cm to 16 cm. Discontinuity of the hepatic surface was seen in 11 cases. In eight cases, CT images during the arterial phase showed a non-enhancing low attenuating lesion with focal discontinuity and peripheral rim enhancement. Seven cases showed separation of tumour content from the peripheral enhancing rim and intraperitoneal rupture of tumour content into the perihepatic space. Because of the similar appearance to an enucleated orbital globe with remaining sclera, this was termed the "enucleation sign". As well as ruptured masses, 10 cases with non-ruptured masses also showed a non-enhancing low attenuating pattern. Seven cases showed a haematoma with high attenuation around the ruptured mass. The peripheral location, protruding contour, discontinuity of the hepatic surface and surrounding haematoma are helpful signs in the diagnosis of ruptured HCC. The "enucleation sign" may be a characteristic finding in ruptured HCC.PMID: 11718385(full text)
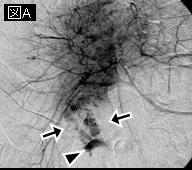
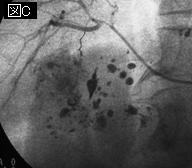
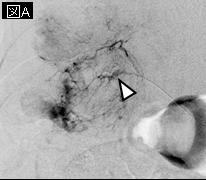
文献考察2):肝細胞癌破裂154例(全肝細胞癌の9%).死亡率は38%,予後不良因子は来院時ショック,貧血,黄疸と進行性手術不可能例.
J Clin Oncol. 2001 Sep 1;19(17):3725-32.
Management of spontaneous rupture of hepatocellular carcinoma: single-center experience.
Liu CL, Fan ST, Lo CM, Tso WK, Poon RT, Lam CM, Wong J.
PURPOSE: To report the management of patients with spontaneous rupture of hepatocellular carcinoma (HCC) in a single center over a 10-year period and to evaluate a two-stage therapeutic approach. PATIENTS AND METHODS: A retrospective study was performed on all 1,716 patients with HCC who presented from 1989 to 1998. The two-stage therapeutic approach to manage ruptured HCC consisted of initial management by conservative method, hemostasis by transarterial embolization (TAE) or surgical means, followed by second-stage hepatic resection or transarterial oily chemoembolization (TOCE). Results of definitive treatment were compared with patients with no history of rupture during the same study period. RESULTS: During the study period, 154 patients (9%) had spontaneous HCC rupture. Initial intervention to control bleeding included TAE in 42 patients, surgical hemostasis in 35 patients, and conservative management only in 53 patients. The 30-day mortality rate was 38%. Independent factors on presentation affecting 30-day mortality were shock on admission, hemoglobin, serum total bilirubin, and known diagnosis of inoperable tumor. After initial stabilization and clinical evaluation, 33 patients underwent hepatic resection and 30 patients received TOCE. Median survival of the hepatectomy patients was 25.7 months; that of the TOCE patients was 9.7 months. Compared with patients with no rupture, survival after hepatectomy (25.7 months v 49.2 months, P =.003) was inferior but still substantially long, whereas survival after TOCE was comparable (9.7 months v 8.7 months, P =.904). CONCLUSION: Early mortality of spontaneous rupture of HCC was dependent on prerupture disease state, liver function, and severity of bleeding. Although it was a catastrophic presentation, prolonged survival could be achieved in selected patients with second-stage hepatic resection or TOCE.PMID: 11533094
|