|
文献考察1):輪状膵(annular pancreas)
【膵の画像診断 最近の押さえどころ】 膵先天異常の画像診断
Author:永山雅子(倉敷中央病院), 渡邊祐司, 奥村明, 天羽賢樹, 中下悟, 上野敏克, 勝部敬, 菅剛, 辰村愛, 百々義廣
Source:画像診断(0285-0524)22巻6号 Page654-661(2002.05)
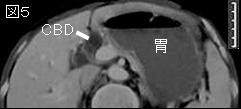
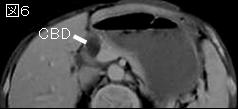
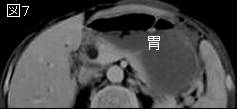
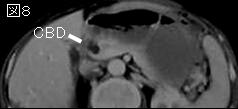
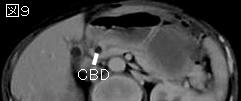
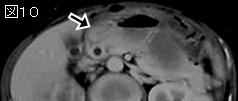
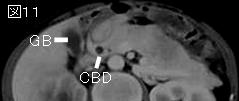
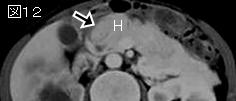
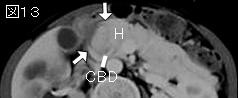
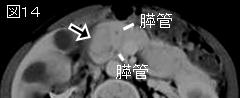
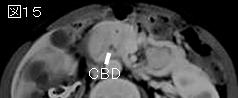
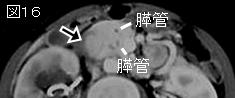
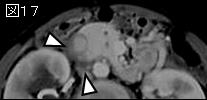
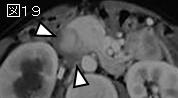
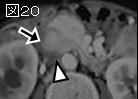
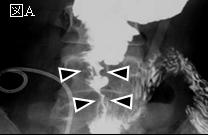
要旨.輪状膵:膵組織の一部が,十二指腸を完全あるいは不完全に取り囲む発生異常である. 約半数は小児期(大部分は新生児期)に発症し, 約半数は成人期に発症する.高度の狭窄例では, 通常新生児期に嘔吐で発症する. 年長児や成人では, 心窩部痛, 食後腹部膨満感, 吐き気, 嘔吐などを呈する.傍膨大部十二指腸潰瘍, 膵炎の発生率が増加し,閉塞性黄疸を生じることもある. 膵炎は, 通常, 輪状膵部と膵頭部に限局する. 単純CTでは十二指腸の壁肥厚像を示すが, 確定診断は難しい. ダイナミックCT早期相では, 膵頭部と連続し, 十二指腸を完全あるいは不完全に取り囲み, 膵と同等の強い造影効果を示す輪状あるいは舌状構造として描出される.
文献考察2):成人の十二指腸先天異常,17年間で29例の経験.男女比は10:19,平均年齢は52歳.病変は十二指腸膜様閉塞20例,輪状膵7例と両病変とも存在した例が2例.
Arch Surg. 2001 May;136(5):576-84.
Congenital duodenal anomalies in the adult.
Ladd AP, Madura JA.
BACKGROUND: Duodenal anomalies are defects in embryologic development and usually present as gastric outlet obstruction in infancy or early childhood. Occasionally, they remain asymptomatic until adulthood and, because they are unusual, may not be diagnosed. HYPOTHESIS: Based on current experience and review of the literature, recognition of diagnosis and the preferred methods of treatment of duodenal anomalies can be recommended. DESIGN: Retrospective study of congenital duodenal anomalies in adults. SETTING: Tertiary care university medical center. PATIENTS: Twenty-nine patients were observed and treated between 1983 and 1999 (19 women and 10 men; mean +/- SD age, 52 +/- 16 years). Twenty patients had duodenal webs, 7 had annular pancreata, and 2 had both. Nausea, vomiting, abdominal pain, and weight loss were predominant symptoms in all groups. Peptic ulceration occurred in 13 of 20 patients with webs but in none of those with annular pancreata or combined anomaly. MAIN OUTCOME MEASURES: Surgical outcomes including postoperative complications, deaths, and resolution of preoperative symptoms. RESULTS: The treatment for patients with duodenal webs was transduodenal web excision and duodenoplasty in 19 of 22. Patients with annular pancreata were treated by transection of the annulus and duodenoplasty (n = 4) and proximal duodenal bypass (n = 3). There were no operative deaths, but 44% of patients had some complications. No pancreatic fistulas occurred in patients who had division of an annular pancreas. Outcome was considered excellent or good in 17 of 20 patients with duodenal webs, 4 of 7 with annular pancreata, and 2 of 2 with the combined anomaly. CONCLUSIONS: Duodenal anomalies are rare in adults. Duodenal webs are best managed by transduodenal excision and duodenoplasty. Annular pancreas is generally best treated by duodenal bypass to the distal duodenum or the jejunum. Annulus division can be carried out if the annulus is extramural, without duodenal stenosis, and if access to the pancreaticobiliary sphincters is necessary.PMID: 11343551
|