|
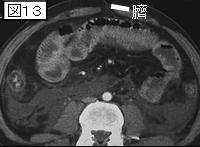
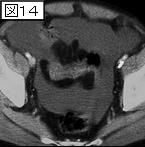
文献考察1):急性膵炎の合併症率と死亡率はBalthazarのCTSI(Expertコース症例52の解説:表)0〜3:42%と2%,4〜6:81%と18%,7〜10:100%と33%で,CTSIは予後判定に極めて有用.
J Am Coll Surg. 2005 Oct;201(4):497-502.
Computed tomography severity index is an early prognostic tool for acute pancreatitis.
Vriens PW, van de Linde P, Slotema ET, Warmerdam PE, Breslau PJ.
BACKGROUND: Acute pancreatitis is a severe disease with unpredictable course and outcomes. It is especially hard to identify early those patients who will have a fulminant course. In a prospective observational study, we tested the hypothesis that the CT Severity Index (CTSI), established within 48hours after admission, is prognostic for morbidity and mortality and can predict the necessity for admission to an ICU. STUDY DESIGN: From January 1994 to October 2002, all patients with the diagnosis of first time acute pancreatitis underwent spiral CT with intravenous contrast within 48hours of admission. The extent of inflammation and necrosis was assessed to define the CTSI. Patients were initially managed in an ICU in a standardized fashion. Complications and mortality were registered in a systematic manner. RESULTS: Seventy-nine patients were admitted with acute pancreatitis. The overall complication rate was 57%; mortality was 9%. In patients with a CTSI of 0 to 3, these rates were 42% and 2%, respectively; in those with CTSI of 4 to 6, 81% and 19%, respectively; and in those with CTSI of 7 to 10, 100% and 33%, respectively. Outcomes of subsequent CT scans did not alter the initial prognosis. Early CTSI correlated well with the incidence of complications, sepsis, mortality, and necessity for ICU admission. CONCLUSIONS: Acute pancreatitis is associated with marked morbidity and mortality. Initial admission to an ICU and standardized conservative treatment are justified for all patients. Early establishment of the CTSI is an excellent prognostic tool for complications and mortality. Patients with a CTSI of 0 to 3 can safely be discharged from the ICU.PMID: 16183486
文献考察2):CTSIは重症患者の予後判定に有用.CTSI値6以上だと,5以下のグループと比較して死亡率は8倍,長期入院の可能性が17倍高く,手術(necrosectomy)の頻度も10倍となる.
Am J Surg. 2000 May;179(5):352-5.
Computed tomography severity index is a predictor of outcomes for severe pancreatitis.
Simchuk EJ, Traverso LW, Nukui Y, Kozarek RA.
BACKGROUND: In a small group of patients with acute pancreatitis, Balthazar and Ranson demonstrated the applicability of computed tomography (CT) criteria to predict mortality. Building upon their work with a larger group of patients with acute pancreatitis, we set out not only to demonstrate that the CT severity index can predict death, but also length of hospital stay and need for necrosectomy. METHODS: We reviewed all patients admitted to our hospital in the years 1992 to 1997 with a primary diagnosis of acute pancreatitis. Entrance criteria required that a CT scan had been performed during the hospitalization. The index CT scan was used to determine a CT severity index (the CTSI of Balthazar and Ranson). Outcomes measured were death, length of stay (LOS), and need for necrosectomy (NEC). Statistical analysis was performed using Fisher's exact and chi-square tests where appropriate. RESULTS: Between the years 1992 to 1997, 886 patients had 1,774 admissions for acute pancreatitis, of which 268 had a CT scan performed and were entered into our study. These 268 patients had a mean age of 57 years, a mean LOS of 16 days (1 to 118), and a mean CTSI of 3.9 (0 to 10). Overall mortality was 4% (n = 11). A CTSI >5 significantly correlated with death (P = 0.0005), prolonged hospital stay (P 5 were 8 times more likely to die, 17 times more likely to have a prolonged hospital course, and 10 times more likely to undergo necrosectomy than their counterparts with CT scores
|











;){kind=link}