|
文献考察:感染性膵壊死と膵膿瘍
1)【肝胆膵の救急画像】 急性膵炎 CTを中心とする病態把握
Author:片岡慶正(京都府立医科大学 消化器病態制御学), 高田龍介, 金光大石, 伊藤令子, 元好朋子, 阪上順一, 光藤章二, 岡上武
Source:消化器画像(1344-3399)6巻2号 Page261-272(2004.03)
2)肝胆膵領域の画像診断】 膵疾患 急性膵炎の画像診断 自己免疫性膵炎を含む(解説/特集)
Author:上野恵子(東京女子医科大学附属第二病院 放射線科), 寺田茂彦, 藤村幹彦, 木村文子
Source:臨床放射線(0009-9252)49巻11号 Page1507-1520(2004.10)
3)Jacobs JE, Birnbaum BA.
Computed tomography evaluation of acute pancreatitis.
Semin Roentgenol. 2001 Apr;36(2):92-8. Review. PMID: 11329661
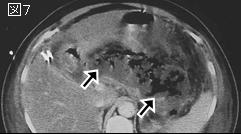
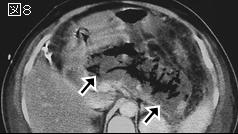
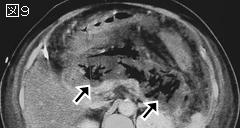
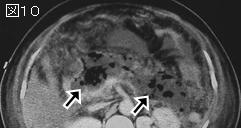
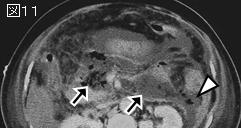
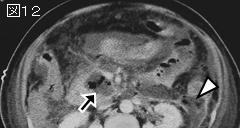
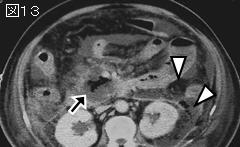
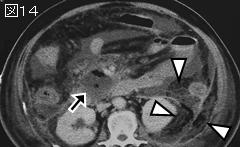
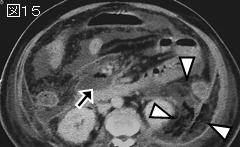
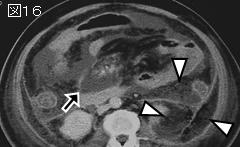
3文献のまとめ:感染性膵壊死(infected pancreatic necrosis).急性膵炎の細菌感染は7〜12%に起こり,死亡原因の80%を占める.感染性膵壊死は発症後1〜3週と比較的早期に認められ,感染の原因は結腸からのbacterial translocationであり,死亡率は39〜67%と高く膵膿瘍の2倍である.ガスを含まない限りCT診断は困難で,診断にはfine needle aspirationと吸引された液の培養が必要である.壊死を伴う重症膵炎では細菌感染は時間の経過とともに増加し,発症後3週では60%に達するとの報告もある.感染性膵壊死は敗血症や多臓器不全を引き起こし,予後は不良で,外科的治療の適応である.
膵膿瘍(pancreatic abscess)は,膵および膵に隣接した限局性の膿瘍であり,内部に壊死組織が無いか,あってもごくわずかである.急性膵炎の約3%に起こる.膵炎発症後4週間目以降に起こす例が多く,30〜40%にガスを含む.最近は経皮的ドレナージのみで治療可能な例が増えてきた.ガスを含まない例では非感染性液貯留との鑑別はCTだけでは困難である.
4)膵膿瘍:経皮的ドレナージで成功率86%
AJR Am J Roentgenol. 1997 Apr;168(4):979-84.
Percutaneous radiologic drainage of pancreatic abscesses.
vanSonnenberg E, Wittich GR, Chon KS, D'Agostino HB, Casola G, Easter D, Morgan RG, Walser EM, Nealon WH, Goodacre B, Stabile BE.
OBJECTIVE: The purpose of our study was to review and report the patient selection, techniques, and results of percutaneous drainage of pancreatic abscesses by retrospective review. MATERIALS AND METHODS: Fifty-nine patients (46 men and 13 women) with a mean age of 44 years old had 80 pancreatic abscesses that were drained percutaneously under radiologic guidance (CT, n = 77; sonography, n = 2; and fluoroscopy, n = 1). Abscesses had a wide spectrum of causes, with alcoholic pancreatitis being most common, trauma second most common, and gallstones third. Ten patients had undergone surgery for pancreatic necrosis or abscess. Patients with pancreatic pseudocysts, necrosis, or acute fluid collections were excluded from this study. RESULTS: Of the 59 patients, 51 (86%) were cured with percutaneous drainage and antibiotic therapy. Of the patients who were not cured with percutaneous drainage, seven required surgery and one underwent repeat percutaneous drainage. In the 59 patients, complications included non-life-threatening bleeding in three patients. Ten of 59 patients (17%) had fistulas that spontaneously formed into the gastrointestinal tract. The duration of catheterization ranged from 4 to 119 days, with a mean duration of 33 days. The rate of mortality at 30 days after completion of percutaneous drainage was 8% (5 of 59). CONCLUSION: Percutaneous drainage was an effective therapy for this defined group of patients with pancreatic abscesses. Factors leading to the relatively high success rate described in this study likely included selection of patients; catheters of adequate size, number, and location; careful follow-up with appropriate catheter manipulations; and an integrated, cooperative approach whereby surgeons were willing to permit drainage to effect its benefits, rather than operating prematurely.PMID: 9124154
|