|
文献考察:急性胆嚢炎のCT所見
1)AJR Am J Roentgenol. 1996 May;166(5):1085-8.
CT evaluation of acute cholecystitis: findings and usefulness in diagnosis.
Fidler J, Paulson EK, Layfield L.
OBJECTIVE: The purpose of our study was to describe the CT findings of acute cholecystitis and apply previously proposed CT criteria for its diagnosis. MATERIALS AND METHODS: We retrospectively reviewed CT scans of 29 patients with proven acute cholecystitis. Scans were reviewed for gallstones, gallbladder distension, bile density, wall thickening, pericholecystic fluid, subserosal edema, pericholecystic stranding, and sloughed membranes. Previously published criteria were applied to determine the percentage of patients that met positive criteria for acute cholecystitis. RESULTS: The most common CT findings, in decreasing order of frequency, were wall thickening (n = 17), pericholecystic stranding (n = 15), distension (n = 12), pericholecystic fluid (n = 9), subserosal edema (n = 9), high-attenuation bile (n = 7), and sloughed membranes (n = 1). Of the 29 cases of acute cholecystitis, 15 met previously published CT criteria. CONCLUSION: CT can be useful in diagnosing acute cholecystitis. Common CT findings of acute cholecystitis include wall thickening, pericholecystic stranding, distention, high-attenuation bile, pericholecystic fluid, and subserosal edema. When these findings are present, the diagnosis of acute cholecystitis can be suggested. However, previously published CT criteria failed to identify a significant number of patients with acute cholecystitis.PMID: 8615248
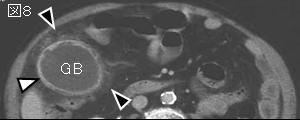
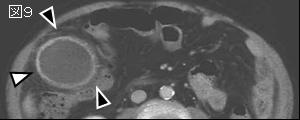
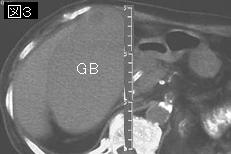
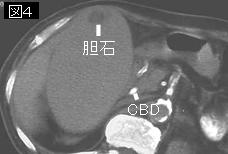
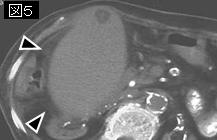
追記:胆嚢の腫大は短軸5cm以上,長軸8cm以上,壁肥厚は4mm以上.major criteria:壁肥厚,胆嚢周囲液貯留または脂肪組織濃度上昇,漿膜下浮腫,壁内ガス,剥離し胆嚢内に浮遊している粘膜像.minor criteria:腫大,高濃度の胆汁(sludge:胆泥).major criteriaが2つ,または2つのminor criteriaと1つのmajor criteriaがあれば急性胆嚢炎と診断する.
2)Semin Ultrasound CT MR. 2000 Feb;21(1):56-63.
Acute cholecystitis: CT findings.
Paulson EK.
Some patients with acute cholecystitis may have symptoms suggestive of an abscess or other intra-abdominal inflammation and, therefore, may be referred for a CT of the abdomen. This report reviews the pathophysiology, clinical presentation, and CT findings of acute cholecystitis (gallstones, wall thickening, distention, pericholecystic fluid, and pericholecystic stranding). Pitfalls and complications of the diagnosis are discussed. Those scenarios where CT may prove superior to ultrasound or hepatobiliary scintigraphy are highlighted.PMID: 10688067
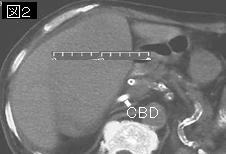
追記:胆嚢腫大は4〜5cm以上,壁肥厚は3mm以上とするが,胆嚢壁肥厚は肝炎,低蛋白血症,心不全などでも見られるので注意を要する.
3)【肝胆膵領域の画像診断】 胆嚢疾患 胆石症および急性胆嚢炎診断における諸問題
Author:岡田真広(国立病院機構東京医療センター 放射線科), 大熊潔
Source:臨床放射線(0009-9252)49巻11号 Page1455-1466(2004.10)
要旨:急性胆嚢炎の診断.超音波検査による所見は,胆嚢が腫大・緊満し(横径が4cm以上),胆嚢壁が一様に厚くなり(3mm以上),胆嚢内腔にdebrisがあり,周囲に液体貯留,漿膜下浮腫を反映したsonolucent layerのため3層構造となる.その他には検査時に探触子で圧迫すると痛みを伴うsonographic Murphy sign ,壁内気腫,遠位胆嚢管の閉塞を示唆する肝内胆管の拡張である.
4)Radiol Clin North Am. 2003 Nov;41(6):1203-16.
Ultrasound and CT evaluation of emergent gallbladder pathology.
Bennett GL, Balthazar EJ.
Ultrasound is the initial imaging modality of choice for the evaluation of suspected acute gallbladder disorders, and is often sufficient for correct diagnosis. CT also plays a vital role, however, in the evaluation of acute gallbladder pathology. CT is particularly useful in situations where ultrasound findings are equivocal. CT is also extremely valuable in the assessment of suspected complications of acute cholecystitis, particularly emphysematous cholecystitis, hemorrhagic cholecystitis, and gallbladder perforation, which are often very difficult diagnoses to establish at sonography. If CT is the initial imaging test performed in a patient with abdominal pain of uncertain etiology, recognition of the various disorders described in this article may eliminate the need for further imaging and facilitate appropriate management.PMID: 14661666
|