|
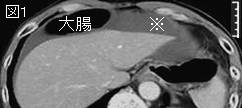
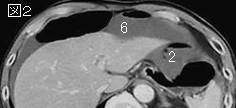
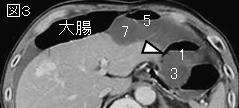
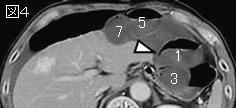
文献考察:腸管嚢腫様気腫症:pneumatosis intestinalis(壁内気腫:intramural gas)
1)Radiology. 1998 Apr;207(1):13-9.
Pneumatosis intestinalis: a review.
Pear BL.
This review illustrates the changing paradigms in the understanding of the pathogenesis of pneumatosis intestinalis. Although many theories have been evoked, pragmatically there appear to be four major clinical and diagnostic imaging considerations. The most common and most emergent life-threatening cause of intramural bowel gas is the result of bowel necrosis due to bowel ischemia, infarction, necrotizing enterocolitis, neutropenic colitis, volvulus, and sepsis. In the stomach, intramural gas can be caused by emphysematous gastritis or ingestion of caustic agents. These situations represent surgical emergencies. Pneumatosis is found secondary to mucosal disruption presumably due to over-distention from peptic ulcer, pyloric stenosis, annular pancreas, and even to more distal obstruction. Disruption can also be caused by ulceration, erosions, or trauma, including the trauma of child abuse. Disruption can also be iatrogenic from intracatheter jejunal feeding tubes, stent perforation, sclerotherapy, or surgical or endoscopic trauma. In these cases, the gas may be focal or linear. Treatment depends on the extent of the disruption and the underlying cause. A more subtle form of mucosal disruption may occur due to mucosal erosions and also to defects in intestinal crypts secondary to acute and subclinical enteritides that allow intraluminal bacterial gas under pressure to percolate into the bowel wall layers, particularly the submucosa (29). Pneumatosis, often linear or cystic in appearance, is seen with increased frequency in patients who are immunocompromised because of steroids, chemotherapy, radiation therapy, or AIDS. In these cases, the pneumatosis may result from intraluminal bacterial gas entering the bowel wall due to increased mucosal permeability caused by defects in bowel wall lymphoid tissue. Clinical and imaging findings are important in the differentiation of this transient pneumatosis from fulminant life-threatening causes in this subset of patients. A pulmonary cause must still be considered in cases of chronic obstructive pulmonary disease, asthma, and cystic fibrosis. It can occur with barotrauma and after chest tube placement. It may relate to increased intrathoracic pressure associated with retching and vomiting. The possibility remains that occasionally the origin of pneumatosis intestinalis will remain cryptogenic--caused but unexplained.PMID: 9530294
追記:病因分類は表1.腸管壊死以外の原因は多く多様である.
2)AJR Am J Roentgenol. 2001 Dec;177(6):1319-23.
Pneumatosis intestinalis and portomesenteric venous gas in intestinal ischemia: correlation of CT findings with severity of ischemia and clinical outcome.
Wiesner W, Mortele KJ, Glickman JN, Ji H, Ros PR.
OBJECTIVE: The purpose of this study was to analyze the correlation between pneumatosis or portomesenteric venous gas, or both, the severity of mural involvement, and the clinical outcome in patients with small- or large-bowel ischemia. MATERIALS AND METHODS: CT scans of 23 consecutive patients presenting with pneumatosis or portomesenteric venous gas caused by bowel ischemia were reviewed. The presence and extent of both CT findings were compared with the clinical outcome in all patients and with the severity and extent of ischemic bowel wall damage as determined by surgery (15 patients), autopsy (three patients), or follow-up (five patients). RESULTS: Seven patients showed isolated pneumatosis, and 16 patients showed portomesenteric venous gas with or without pneumatosis (11 and five patients, respectively). Pneumatosis and portomesenteric venous gas were associated with transmural bowel infarction in 14 (78%) of 18 patients and 13 (81%) of 16 patients, respectively. Nine patients (56%) with portomesenteric venous gas died. Of seven patients with infarction limited to one bowel segment (jejunum, ileum, or colon), only one patient (14%) died, whereas of the 10 patients with infarction of two or three bowel segments, eight patients (80%) died. CONCLUSION: CT findings of pneumatosis intestinalis and portomesenteric venous gas due to bowel ischemia do not generally allow prediction of transmural bowel infarction, because they may be observed in patients with only partial ischemic bowel wall damage. The clinical outcome of patients with bowel ischemia with these CT findings seems to depend mainly on the severity and extent of their underlying disease.PMID: 11717075
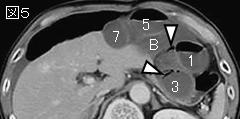
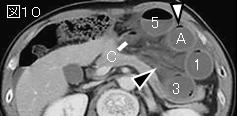
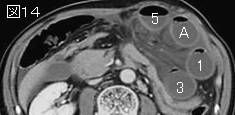
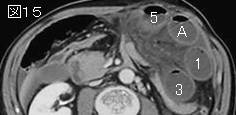
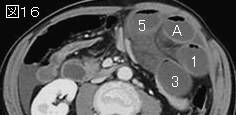
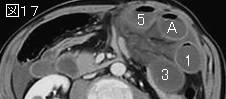
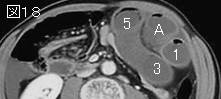
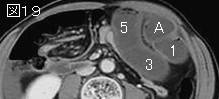
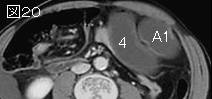
上記2文献のまとめ:腸管嚢腫様気腫症:pneumatosis (cystoides)intestinalis(壁内気腫:intramural gas)は腸管壁内(粘膜下または漿膜下)に含気性嚢胞を生じるまれな疾患である.本症の病因として,1)細菌説:腸管壁に弱毒性のガス産生菌が進入することにより起こるもの,2)機械説:腸管内圧上昇があり,腸管粘膜の微細な損傷部位より腸管壁内にガスが進入し気腫を形成する,3)肺原説:喘息,慢性気管支炎による咳嗽,胸腔内圧上昇により肺胞破裂が起こり漏れた空気が縦隔気腫となり,後腹膜腔を通って血管壁に沿って腸管壁に達する.
|



;){kind=link}