|
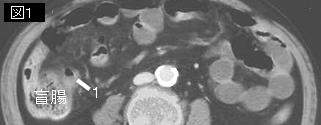
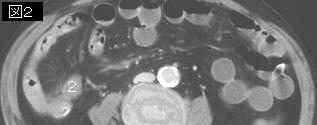
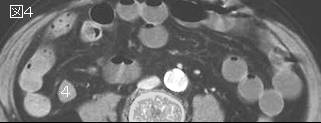
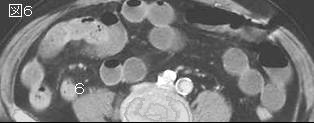
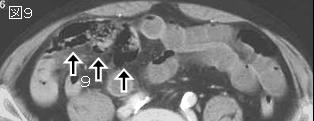
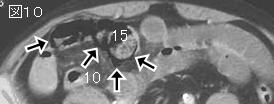
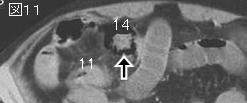
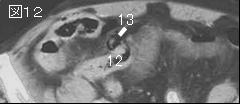
文献考察:腸管嚢腫様気腫症pneumatosis intestinalis(壁内気腫intramural gas)
Radiology. 1998 Apr;207(1):13-9.
Pneumatosis intestinalis: a review.
Pear BL.
This review illustrates the changing paradigms in the understanding of the pathogenesis of pneumatosis intestinalis. Although many theories have been evoked, pragmatically there appear to be four major clinical and diagnostic imaging considerations. The most common and most emergent life-threatening cause of intramural bowel gas is the result of bowel necrosis due to bowel ischemia, infarction, necrotizing enterocolitis, neutropenic colitis, volvulus, and sepsis. In the stomach, intramural gas can be caused by emphysematous gastritis or ingestion of caustic agents. These situations represent surgical emergencies. Pneumatosis is found secondary to mucosal disruption presumably due to over-distention from peptic ulcer, pyloric stenosis, annular pancreas, and even to more distal obstruction. Disruption can also be caused by ulceration, erosions, or trauma, including the trauma of child abuse. Disruption can also be iatrogenic from intracatheter jejunal feeding tubes, stent perforation, sclerotherapy, or surgical or endoscopic trauma. In these cases, the gas may be focal or linear. Treatment depends on the extent of the disruption and the underlying cause. A more subtle form of mucosal disruption may occur due to mucosal erosions and also to defects in intestinal crypts secondary to acute and subclinical enteritides that allow intraluminal bacterial gas under pressure to percolate into the bowel wall layers, particularly the submucosa (29). Pneumatosis, often linear or cystic in appearance, is seen with increased frequency in patients who are immunocompromised because of steroids, chemotherapy, radiation therapy, or AIDS. In these cases, the pneumatosis may result from intraluminal bacterial gas entering the bowel wall due to increased mucosal permeability caused by defects in bowel wall lymphoid tissue. Clinical and imaging findings are important in the differentiation of this transient pneumatosis from fulminant life-threatening causes in this subset of patients. A pulmonary cause must still be considered in cases of chronic obstructive pulmonary disease, asthma, and cystic fibrosis. It can occur with barotrauma and after chest tube placement. It may relate to increased intrathoracic pressure associated with retching and vomiting. The possibility remains that occasionally the origin of pneumatosis intestinalis will remain cryptogenic--caused but unexplained.PMID: 9530294
|






;){kind=link}