|
文献考察1):小児急性虫垂炎,穿孔率が高い.
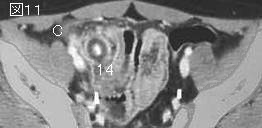
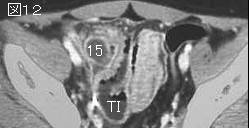
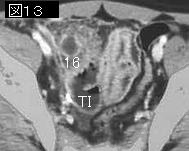
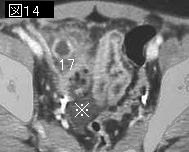
【小児虫垂炎 診断・治療の現況】 検査値ならびに理学所見からの診断
Author:黒田達夫(国立小児病院), 嶋寺伸一, 森川信行, 中野美和子, 中目和彦, 佐伯守洋
Source:小児外科(0385-6313)33巻5号 Page462-465(2001.05)
Abstract:当院における急性虫垂炎症例について理学的所見,X線所見,白血球数,CRP値など最も一般的な項目を選んで検討を行った.小児の急性虫垂炎は特に低年齢発症の症例では診断が難しく,かつ進行が早いため穿孔率が高い臨床像が示唆された.理学的所見や検査値において特異性の高いものはなく,これらを総合的に判断して診断する必要があると考えられた.
追記:穿孔例は30%,5歳以下だと50%.
文献考察2):感染性腸炎のmanagement.
Guerrant RL, Van Gilder T, Steiner TS, Thielman NM, Slutsker L, Tauxe RV, Hennessy T, Griffin PM, DuPont H, Sack RB, Tarr P, Neill M, Nachamkin I, Reller LB, Osterholm MT, Bennish ML, Pickering LK; Infectious Diseases Society of America.
Practice guidelines for the management of infectious diarrhea.
Clin Infect Dis. 2001 Feb 1;32(3):331-51.PMID: 11170940
要旨:下痢とは,便の性状が軟便または水様便で,1日3回以上の排便をいう.急性下痢とは期間が14日以内,持続性下痢とは14日以上続く下痢である.30日以上持続する下痢を慢性下痢という著者もいる.感染性下痢のmanagementのガイドラインは図を参照.
文献考察3):小児急性虫垂炎,USまたはCT検査を減らす方法.
Pediatrics. 2004 Jan;113(1 Pt 1):24-8.
Selective imaging strategies for the diagnosis of appendicitis in children.
Garcia Pena BM, Cook EF, Mandl KD.
BACKGROUND: We previously reported an appendiceal imaging protocol in which children with equivocal clinical presentations for acute appendicitis undergo ultrasonography (US) followed by computed tomography (CT). However, risk groups of children who would benefit most from imaging studies have not been established. OBJECTIVE: To define and test selective imaging guidelines to increase diagnostic accuracy and reduce unnecessary testing for children with suspected appendicitis. METHODS: We modeled outcomes under 3 different management guidelines. Patients were risk-stratified by a recursive partitioning analysis of a retrospective cohort. Subjects included children with equivocal presentations of acute appendicitis evaluated between January 1996 and December 1999. By using recursive partitioning, 3 risk groups were identified: low, medium, and high risk for acute appendicitis. Three imaging guidelines were defined. Under the first guideline, representing standard clinical practice at Children's Hospital Boston at the time of the study, all children with equivocal signs and symptoms for acute appendicitis undergo US first. If the US is positive, the child proceeds to appendectomy. If the US is negative, the child undergoes CT. Under guideline 2, low-risk children undergo US and, if negative, are discharged from the hospital. High-risk children undergo CT, and medium-risk children undergo US followed by CT. Under the third guideline, low-risk children undergo no imaging and are admitted for observation. High-risk children proceed directly to appendectomy without imaging studies. Medium-risk children undergo US followed by CT. Clinical outcomes and the number of imaging studies performed were modeled under current practice and under each guideline. RESULTS: Identified were 1401 cases of equivocal appendicitis; 958 (68.4%) with complete data. The mean age was 11 +/- 4.3 years. Of 958 children, 588 (61.4%) had acute appendicitis. One hundred forty-three patients were in the low-risk group, defined as neutrophils ≦67%, bands . Fifteen (10%) children had appendicitis. Two hundred twenty-five were high-risk for appendicitis defined as neutrophils >67%, white blood cell count >10,000/mm(3), guarding, and abdominal pain >13 hours. Of these, 202 (90%) had appendicitis. Under guideline 1, there were 22 negative appendectomies, 35 missed or delayed diagnoses, and 958 USs and 673 CT scans performed. Under guideline 2, there would have been 23 negative appendectomies, 36 missed or delayed diagnoses, and 733 USs and 637 CT scans performed. Under guideline 3, there would have been 36 negative appendectomies, 37 missed or delayed diagnoses, and 590 USs and 412 CT scans performed. CONCLUSIONS: Selective imaging guidelines can reduce the number of radiographic studies performed with minimal diminution in accuracy of diagnosis of pediatric appendicitis.PMID: 14702442(full text)
|




;){kind=link}