|
文献考察:腹膜偽粘液腫(pseudomyxoma peritonei)
1)Turnage RH,Li BD,McDonald JC.
Abdominal wall,Umbilicus,Peritoneum,Mesenteries,Omentum,and Retroperitoneum.
Townsend: Sabiston Textbook of Surgery, 17th ed., page:1187,2004.Elsevier Saunders,Philadelphia.
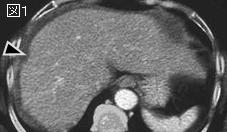
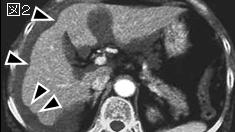
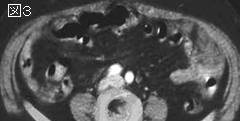
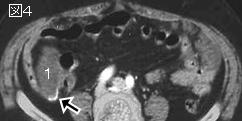
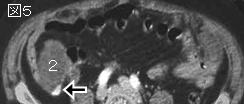
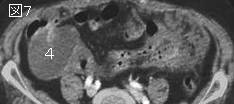
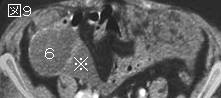
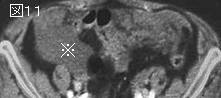
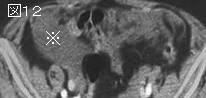
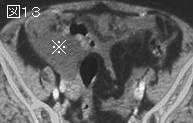
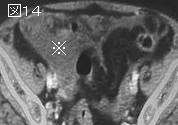
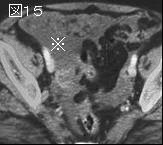
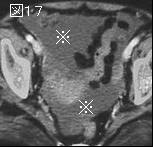
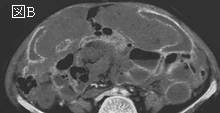
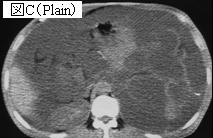
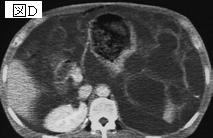
要旨:破裂性の卵巣癌か虫垂癌から生じるまれな腹腔内の悪性疾患である.腹膜にムチン産生腫瘍細胞が着床し,腹腔内には粘稠性の半固形の粘液を認める.50〜70歳代の女性に多い.CTでは多房性の嚢胞状腫瘤を認め,腸管は背側に圧排される.肝臓や脾臓では着床した腫瘍塊による圧排像(scalloping)を認めることが特徴である.low grade malignancyだから経過は長いことが多いが,5年生存率は50%,10年生存率は20%程度である.
2)Clin Radiol. 2002 Jul;57(7):608-13.
CT in pseudomyxoma peritonei: a review of 17 cases.
Sulkin TV, O'Neill H, Amin AI, Moran B.
AIM: To describe the computed tomography (CT) findings in pseudomyxoma peritonei. MATERIALS AND METHOD: Two observers independently and retrospectively reviewed the CT images of 17 consecutive patients (nine women, eight men, mean age 53 years) with histologically proven pseudomyxoma peritonei. RESULTS: Six patients had small volume disease where pseudomyxoma peritonei was present in focal collections in the peritoneal cavity. Eleven had large volume disease that completely, or almost completely, filled the peritoneal cavity. Pseudomyxoma peritonei is characterized by low attenuation mucinous ascites on CT. Areas of high attenuation, septae and calcification are seen more commonly within it as the volume of disease increases. The pattern of accumulation of pseudomyxoma peritonei follows the normal flow of peritoneal fluid. It initially seeds at sites of relative stasis and as large volume disease develops it fills the remaining spaces in the peritoneal cavity and pressure effects dominate imaging. Pseudomyxoma peritonei may extend into hernial orifices or the pleural cavity. CONCLUSION: Pseudomyxoma peritonei is difficult to diagnose clinically. However, the pattern of accumulation of disease is predictable and can be recognized on CT. PMID: 12096860
3)Br J Surg. 2000 Oct;87(10):1414-8.
Clinical presentation of the Pseudomyxoma peritonei syndrome.
Esquivel J, Sugarbaker PH.
BACKGROUND: Pseudomyxoma peritonei syndrome is characterized by a gradual expansion of mucoid tumour and fluid at specific sites within abdominopelvic regions as a result of a perforated appendiceal adenoma. The aim was to analyse the presenting symptoms and signs of patients with this condition. METHODS: Of 410 patients with appendiceal tumours 217 had the diagnosis of pseudomyxoma peritonei syndrome with histological confirmation. A retrospective review of the clinical characteristics that determine presentation was performed. RESULTS: Overall, suspected acute appendicitis was the most common presentation (27 per cent). For women the diagnosis was most commonly made while being evaluated for an ovarian mass (39 per cent). Increasing abdominal girth was the second most common presentation overall (23 per cent). Thirty patients (14 per cent) presented with new-onset hernia, of which the majority (26) were inguinal hernias. CONCLUSION: Consideration of appendicitis, increased abdominal girth, ovarian mass and new-onset hernia as caused by this syndrome may facilitate diagnosis and definitive treatment.PMID: 11044169
|