|
文献考察:穿孔性虫垂炎のCT所見
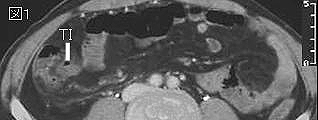
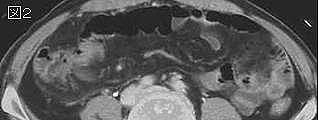
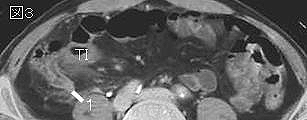
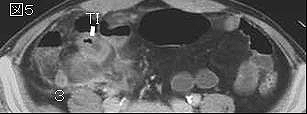
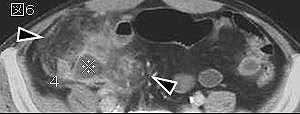
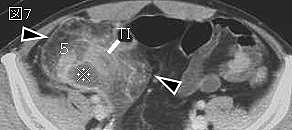
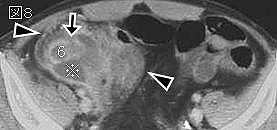
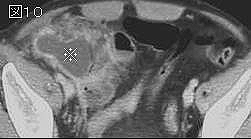
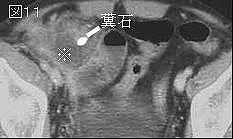
下記文献のまとめ.虫垂炎穿孔のCT所見は,急性虫垂炎の所見に加えて,1)膿瘍形成,2)腸管外遊離ガス,3)虫垂外糞石,4)広範囲のphlegmon(蜂巣炎),5)虫垂壁の欠損像,6)広範囲の腹膜・筋膜の造影・肥厚,7)大量の腹水または液貯留,8)麻痺性イレウス,9)虚脱した虫垂,10)盲腸,回腸末端の壁肥厚.1〜5が特異性が高い.
1)Am J Emerg Med. 2005 Jan;23(1):60-6.
Can ruptured appendicitis be detected preoperatively in the ED?
Lin CJ, Chen JD, Tiu CM, Chou YH, Chiang JH, Lee CH, Chang CY, Yu C.
PURPOSE: The purpose of this study is to determine which clinical symptoms/signs and computed tomography (CT) signs can help in distinguishing ruptured from simple appendicitis. MATERIALS AND METHODS: The medical records and CT findings of 202 consecutive patients with surgically proven acute appendicitis were retrospectively reviewed and compared between 2 groups with and without appendiceal rupture. RESULTS: Longer duration of symptoms ( P
2)Clin Imaging. 2004 Nov-Dec;28(6):422-7.
Evaluation of perforated and nonperforated appendicitis with CT.
Yeung KW, Chang MS, Hsiao CP.
Fifty-three patients with 38 cases of perforated appendicitis and 15 cases of appendicitis without perforation were evaluated based on the computed tomography (CT) appearances of appendiceal diameter, phlegmon, abscess, extraluminal air, appendiceal wall enhancement, lateroconal fascial thickening, appendicolith, bowel wall thickening, ascites, ileal wall enhancement, peritoneal enhancement, periappendiceal fluid, omental haziness, retrocecal appendix, intraluminal air, and the combination of intraluminal air and appendicolith. The result of appendiceal diameter was compared using two-sample Student's t test, and the other CT findings were analyzed by Fisher's Exact Test. Our results showed that appendix was larger in caliber in perforated appendix (P
3)Radiology. 2003 Apr;227(1):46-51.
Differentiation of perforated from nonperforated appendicitis at CT.
Horrow MM, White DS, Horrow JC.
PURPOSE: To evaluate the sensitivity and specificity of five computed tomographic (CT) criteria in the differentiation of perforated from nonperforated appendicitis. MATERIALS AND METHODS: CT scans of 94 patients with surgically proven appendicitis were classified on review as showing perforation if one of five CT findings was present. The authors calculated the sensitivity and specificity for each finding by comparing the predicted outcome to the surgical and pathologic outcome. RESULTS: The perforated group comprised 39 patients and the nonperforated group comprised 55 patients. Sensitivity for abscess, phlegmon, extraluminal air, extraluminal appendicolith, and focal defect in enhancing appendiceal wall individually were 36%, 46%, 36%, 21%, and 64%, respectively. Sensitivity for any one of the five findings was 94.9%. Specificities were 100% for all findings except for phlegmon (95%). Groups differed with respect to age: 47 years +/- 19 (mean +/- SD) for perforated appendicitis and 30 years +/- 13 for nonperforated appendicitis (P <.001 groups also differed with respect to appendiceal diameter: mm for perforated appendicitis and nonperforated conclusion: a dedicated search five specific ct findings allowed an overall sensitivity of appendicitis. among specificity focal defect in the enhancing wall achieved highest sensitivity.pmid:>
4)Pediatr Radiol. 2001 Mar;31(3):173-9.
Imaging findings of perforative appendicitis: a pictorial review.
Hopkins KL, Patrick LE, Ball TI.
Appendicitis is common in children. Early diagnosis depends on recognition of characteristic signs and symptoms: right lower quadrant or periumbilical pain, localized tenderness, fever, and leukocytosis. Because these classic features may be difficult to elicit or masked by other complaints, the incidence of perforative appendicitis in children is high. This paper reviews the imaging sequelae with emphasis on CT and sonography findings. Areas of focus include abdominopelvic abscess, peritonitis, pyelephlebitis, pyelethrombosis, and hepatic abscess. Secondary involvement of the urinary and gastrointestinal tracts is also discussed.PMID: 11297081
5)Radiology. 2005 Apr;235(1):89-96. Epub 2005 Mar 4.
Differentiation of nonperforated from perforated appendicitis: accuracy of CT diagnosis and relationship of CT findings to length of hospital stay.
Foley TA, Earnest F 4th, Nathan MA, Hough DM, Schiller HJ, Hoskin TL.
PURPOSE: To determine retrospectively the sensitivity and specificity of computed tomographic (CT) signs in differentiating acute nonperforated appendicitis from perforated appendicitis and to compare CT findings with the length of hospital stay. MATERIALS AND METHODS: Institutional Review Board approval was obtained for this study, and patient informed consent was obtained for record review for research purposes. Two radiologists were blinded to patient identification but were informed that all patients presented to the emergency department with abdominal pain and underwent appendectomy. Radiologists independently reviewed CT images of 86 consecutive patients (45 males, 41 females; mean age, 33.7 years; age range, 8.2-87.1 years) who presented to the emergency department with acute abdominal pain, who underwent CT after initial emergency department assessment, and who underwent appendectomy within the subsequent 24 hours. Individual findings and confidence level for the diagnosis of perforated appendicitis were noted. Consensus interpretation was performed with a third radiologist. The consensus CT findings were correlated with the surgical and pathologic findings by using chi(2) or Fisher exact tests for univariate analysis and logistic regression for multiple variable analysis. Wilcoxon rank sum tests were used to assess the association between consensus CT findings and length of hospital stay. RESULTS: Twenty-one (24%) of the 86 patients had appendiceal perforation. Extraluminal air and either moderate or severe periappendiceal inflammatory stranding were statistically significant independent predictors for perforation (P
|