|
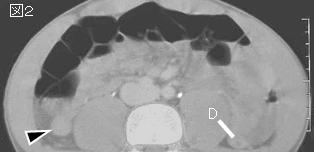
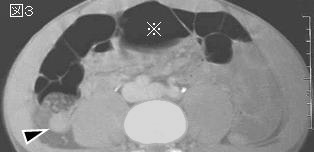
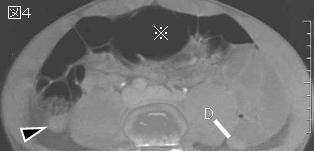
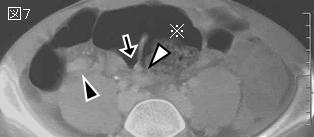
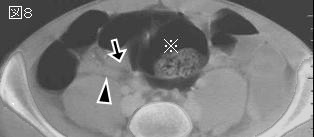
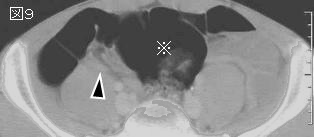
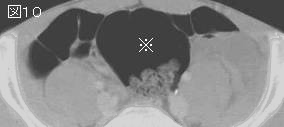
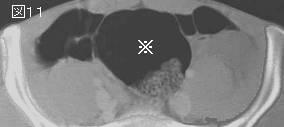
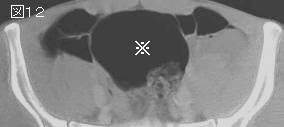
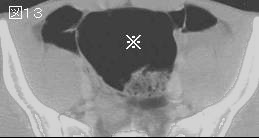
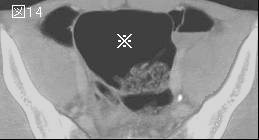
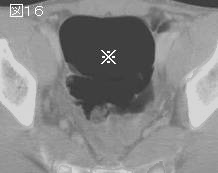
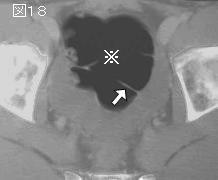
文献考察:盲腸捻転
Am J Surg. 2005 Feb;189(2):211-3.
Operative therapy for cecal volvulus combining resection with colopexy.
Majeski J.
BACKGROUND: Cecal volvulus is an uncommon clinical event. The literature contains many recommended treatments with varied results. STUDY DESIGN: A series of 10 consecutive patients treated by the author was reviewed. Each patient had complete clinical follow-up. The cecal volvulus was resected without detorsion and reperfusion of the volvulus. The intestine was resected using a surgical stapling device, transection of the mesentery at the axial twist, and a stapled anastomosis of the terminal ileum to the remnant of the right colon. Permanent sutures between the colonic tenia and the peritoneum of the right paracolic gutter fixed the remainder of the right colon to prevent recurrence of the volvulus. RESULTS: The author in clinical practice surgically treated a series of 10 consecutive patients with complete follow-up between 1981 to 2004. All patients survived the surgical procedure and were discharged from the hospital. The diagnosis was determined preoperatively in 5 of the 10 patients. Five patients had gangrene of the colon, and two of these patients had perforation. All patients required postoperative intensive care from 2 to 9 days. Five of the 10 patients required ventilator support for 1 to 3 days. Postoperative complications included intraperitoneal bleeding, pneumonia, and surgical incision infection with a subcutaneous abscess. There has been no recurrence of the volvulus in any of these patients. CONCLUSIONS: Ten consecutive cases of cecal volvulus were surgically treated by a uniform resection procedure. The cecal volvulus was not reperfused by detorsion. Reperfusion of ischemic or gangrenous bowel can possibly produce reperfusion injury, metabolic acidosis, intestinal bacterial, and toxin translocation with possible irreversible septic shock. Recurrence of the cecal volvulus was prevented by colopexy of the right colon remnant. Avoidance of reperfusion of the cecal volvulus with resection, primary anastomosis, and colopexy resulted in successful results in a small series in clinical practice.PMID: 15720993
追記:捻転により虚血状態に陥った腸管は捻転解除(detorsion)せず切除すべき.内視鏡的整復に成功した少数例の報告はあるが,成功率は低く,S状結腸捻転と比べ技術的に困難であり,盲腸捻転は壊死に陥っている確率が高いのですぐ手術すべきである.
|