|
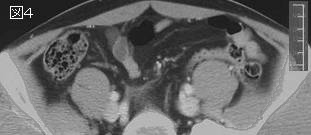
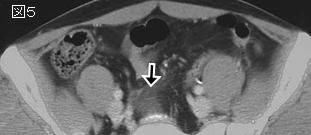
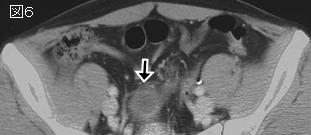
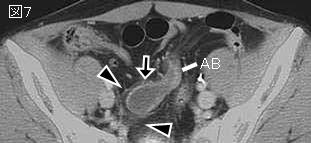
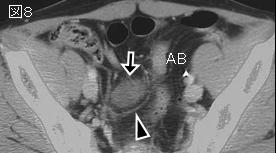
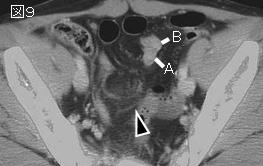
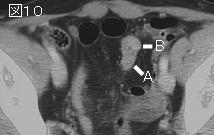
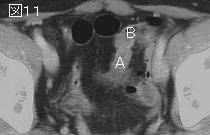
参考文献:Meckel憩室の画像
Radiographics. 2004 Mar-Apr;24(2):565-87.
From the archives of the AFIP. Meckel diverticulum: radiologic features with pathologic Correlation.
Levy AD, Hobbs CM.
Meckel diverticulum is the most common congenital anomaly of the gastrointestinal tract, occurring in 2%-3% of the population. It results from improper closure and absorption of the omphalomesenteric duct. Meckel diverticulum is the most common end result of the spectrum of omphalomesenteric duct anomalies, which also include umbilicoileal fistula, umbilical sinus, umbilical cyst, and a fibrous cord connecting the ileum to the umbilicus. The formation of Meckel diverticulum occurs with equal frequency in both sexes, but symptoms from complications are more common in male patients. Sixty percent of patients come to medical attention before 10 years of age, with the remainder of cases manifesting in adolescence and adulthood. Heterotopic gastric and pancreatic mucosa are frequently found histologically within the diverticula of symptomatic patients. The most common complications are hemorrhage from peptic ulceration, small intestinal obstruction, and diverticulitis. Although the clinical, pathologic, and radiologic features of the complications of Meckel diverticulum are well known, the diagnosis of Meckel diverticulum is difficult to establish preoperatively.PMID: 15026601
|