|
文献考察:右側結腸憩室炎の治療方針.
1)ANZ J Surg. 2001 Nov;71(11):634-6.
Conservative approach is feasible in the management of acute diverticulitis of the right colon.
Chiu PW, Lam CY, Chow TL, Kwok SP.
BACKGROUND: Acute diverticulitis of the caecum and ascending colon is uncommon. Controversies abound as regards the optimal surgical treatment, ranging from appendectomy, diverticulectomy to right hemicolectomy. The aim of the present paper was to review treatment strategy followed by a critical appraisal. METHODS: The case notes of 30 patients with acute diverticulitis of the right colon who were treated at the United Christian Hospital, Hong Kong from 1992 to 1998 were systematically reviewed. The data were subjected to statistical analysis. RESULTS: The median age was 34 years, with a male:female ratio of 1:1.15. All patients presented with acute right lower abdominal pain and localized rebound tenderness. All were diagnosed preoperatively as having appendicitis. The mean duration of symptoms was 2 days (range: 1-6 days). Two treatment groups were identified. Group A (n = 16; 53%) received appendicectomy alone, while group B (n = 14; 47%) underwent diverticulectomy in addition to appendicectomy, including one patient with perforated diverticulitis. Overall, there was no procedure-related morbidity or mortality. Both groups received a similar duration of broad-spectrum antibiotics. All the patients were interviewed by phone after operation to detect any recurrence of symptoms, with a median follow-up interval of 34 months (range: 11-78 months). There was no recurrence of symptoms in group A, which received appendicectomy and antibiotics. The only difference was operative time. CONCLUSION: For non-perforated diverticulitis of the right colon, appendicectomy and intravenous antibiotics without diverticulectomy is the preferred treatment strategy.PMID: 11736820
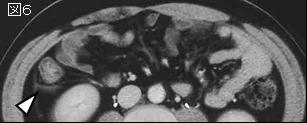
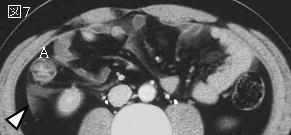
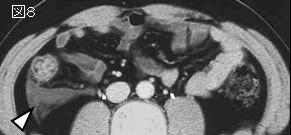
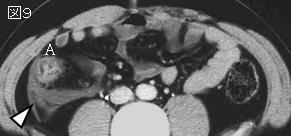
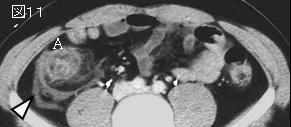
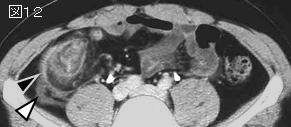
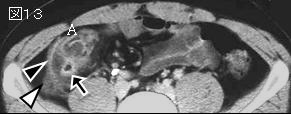
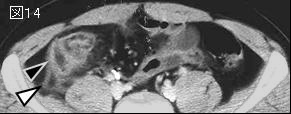
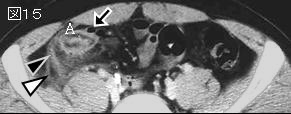
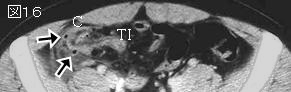
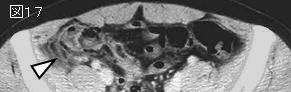
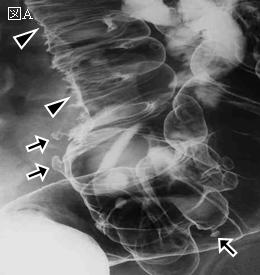
追記:Greaney and Snyder's Classification(Fig.1).GradeI:憩室と周辺だけの炎症,GradeII:腫瘤形成,GradeIII:限局性の穿孔,GradeIV:遊離腹腔内へ穿孔.GradeIIIとGradeIVは手術の適応であることに問題はないが,GradeIとGradeIIに関しては積極的に手術すべき(文献2)と,保存的に治療すべき(文献3)との意見に分かれる.急性虫垂炎と診断し開腹したら,虫垂切除だけ行い,抗生物質投与でいいと著者らはいう.
2)Am J Surg. 2003 Feb;185(2):135-40.
Aggressive resection is indicated for cecal diverticulitis.
Fang JF, Chen RJ, Lin BC, Hsu YB, Kao JL, Chen MF.
BACKGROUND: Because of the difficulties in preoperative diagnosis and controversies in the management, cecal diverticulitis has received much discussion in the literature. There, however, are still many questions that remain unanswered. METHODS: During a 5-year period, 112 patients with a clinical diagnosis of cecal diverticulitis were treated. Twenty-seven patients were excluded because of uncertainty in diagnosis or incomplete data collection, leaving 85 patients as the study group. The diagnosis of cecal diverticulitis was made by pathology, surgical findings, or image study. RESULTS: Nonoperative management was applied to 18 patients initially. Three patients had recurrent diverticulitis during follow up. These patients responded satisfactorily to another course of medical treatment. Laparotomy was performed in 67 patients. Acute appendicitis was the preoperative diagnosis in 47 patients (70%). Of the other 20 patients, 6 received operation because of repeated attack of diverticulitis, 7 had preoperative computed tomography (CT) diagnosis of cecal diverticulitis with perforation, 5 had preoperative diagnosis of cecal tumor, and 2 had medical treatment failure. All these 20 patients received right hemicolectomy. In the 47 patients with a preoperative diagnosis of acute appendicitis, 24 received appendectomy, 9 received diverticulectomy, and 14 received right hemicolectomy. Overall, 34 patients received right hemicolectomy, 9 received diverticulectomy, and 24 received appendectomy only. In the right hemicolectomy group, there were 2 deaths with underlying diseases and 5 complications. In the appendectomy group, there was no postoperative mortality, but in 7 patients recurrent diverticulitis developed. Three of them required right hemicolectomy. CONCLUSIONS: The natural history of cecal diverticulitis varies from benign and self-limiting to fulminant in the oriental population. Less than 40% (32 of 85) of patients were successfully treated with conservative methods initially and had no recurrence during the follow-up period. We recommend aggressive surgical resection for patients with a definite diagnosis. Adjuvant appendectomy without resection of the lesion should be considered only in uncomplicated patients whose diagnosis is in doubt.PMID: 12559443
3)Am J Surg. 2004 Feb;187(2):233-7.
Toward therapeutic guidelines for patients with acute right colonic diverticulitis.
Komuta K, Yamanaka S, Okada K, Kamohara Y, Ueda T, Makimoto N, Shiogama T, Furui J, Kanematsu T.
BACKGROUND: At present, little information is available on the outcome of medical therapy for patients with acute right colonic diverticulitis, and this has meant a gap in constructing guidelines for its treatment. METHODS: The records of patients with acute right colonic diverticulitis at Nagasaki University Graduate School and affiliated hospitals were reviewed and analyzed with the goal of establishing therapeutic guidelines. The time frame of the data analyzed was from 1984 to 2002. RESULTS: Of the 81 patients included in the data, 80 patients who were suffering a first attack were successfully treated with bowel rest and antibiotics. Two of these 80 patients underwent an elective operation at the surgeon's discretion during the original hospitalization and 1 (1.2%) needed an urgent operation. Of the 78 patients who responded to medical therapy, 16 (20.5%) developed recurrent right colonic diverticulitis. All 16 patients who had a second attack were successfully treated with medical therapy. Three of the 16 patients underwent an elective operation during this rehospitalization period. Of the 13 patients who had had a second attack and had responded to medical therapy, there was a third attack in 2 patients (15.4%). Both of these patients were again successfully treated with medical therapy. There has been no morbidity and no mortality related to recurrence to date. The average time from the first attack to us contacting the patient was 35.2 months. CONCLUSIONS: Unlike acute uncomplicated left colonic diverticulitis, our findings indicate that after two documented episodes, medical treatment alone rather than elective surgery may be considered as an effective guideline for the treatment of acute uncomplicated right colonic diverticulitis.PMID: 14769311
|




;){kind=link}