|
文献考察:右側結腸憩室炎のUS・CT診断.
Radiology 1998 Sep;208(3):611-8
Right colonic diverticulitis: US and CT findings--new insights about frequency and natural history.
Oudenhoven LF, Koumans RK, Puylaert JB.
PURPOSE: To evaluate how the use of ultrasonography (US) and computed tomography (CT) has changed insights on the frequency and natural history of right colonic diverticulitis. MATERIALS AND METHODS: Clinical findings, US and CT images, and clinical and surgical records in 44 patients with a final diagnosis of right colonic diverticulitis seen over 11 years were retrospectively studied. RESULTS: Of the 44 patients, three underwent diverticulectomy, and 41 were successfully treated conservatively. Follow-up US demonstrated a consistent change in the pattern of the findings of diverticulitis over time, with eventual spontaneous evacuation of the contents of the inflamed diverticulum into the colonic lumen. Five patients had recurrent symptoms; two of them underwent elective surgery. The frequency of right colonic diverticulitis was one in 34 appendectomies, which is nine times higher than that reported to date. CONCLUSION: Right colonic diverticulitis is more common than has been previously reported. US and CT findings are characteristic and show a consistent pattern of changes over time. The natural history is benign, and surgical intervention can be avoided in the vast majority of patients.PMID: 9722836
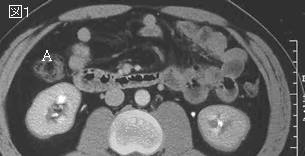
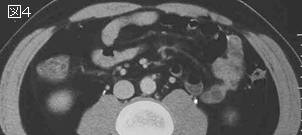
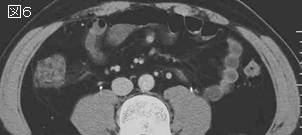
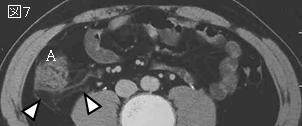
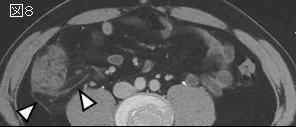
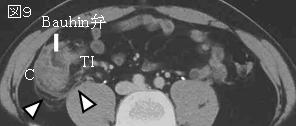
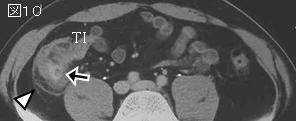
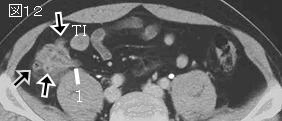
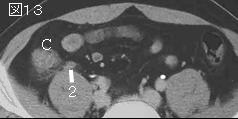
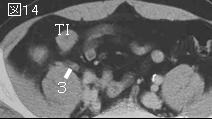
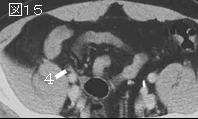
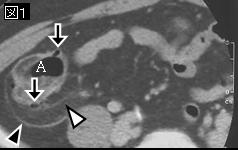
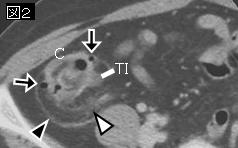
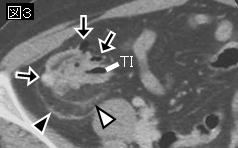
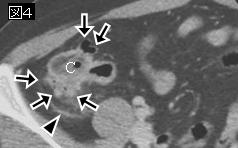
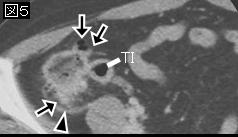
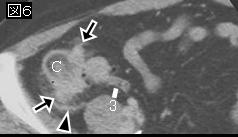
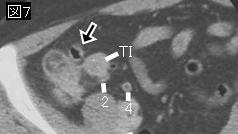
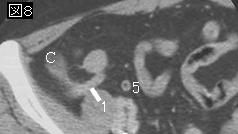
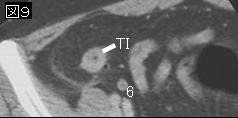
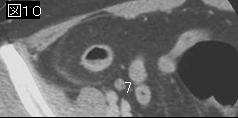
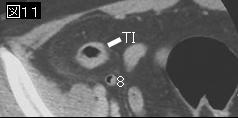
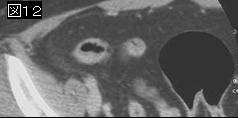
The CT criterion for the diagnosis of right-sided colonic diverticulitis that we used was direct visualization of the diverticulum as an outpouching of the right-sided hemicolon at the level of maximum circumferential wall thickening. The diverticulum was expected to contain gas, fluid, or calcified material with hyperattenuating strands in the surrounding fatty tissue adjacent to the diverticulum. There should be no evidence of appendicitis. Disease in the patients was staged according to the method of Netf and vanSonnenherg for the staging of sigmoid diverticulitis. Stage 0 represents the earliest stage of diverticulitis, with only phlegmonous changes around the diverticulum containing a fecalith (Figs 1). Stage 1 implies the presence of a small pericolonic abscess. We introduce here stage R diverticulitis, a residual stage of the disease after spontaneous evacuation The diverticulum is empty, and the bowel wall thickening and the amount of surrounding inflamed fat have decreased (Fig 1).
Figure 1. Schematic reconstruction of the natural history of right-sided colonic diverticulitis. The starting point is stage 0 inflammation of the diverticulum, which contains a fecalith and is surrounded by inflamed fat that represents mesentery and omentum. There is local, circumferential thickening of the colonic wall. Evacuation of the contents of the diverticulum takes place either directly (stage 0 evolving to stage R) or by means of the intermediate development of a small pericolonic abscess (stage 0 evolving to stage 1 evolving to stage R). The common end point after spontaneous evacuation is stage R, which is characterized by gradual resolution of the inflammatory abnormalities.
|







;){kind=link}