|
文献考察1):経静脈的enhanceによる正常虫垂のCT所見・急性虫垂炎のCT所見
Rowling SE, Jacobs JE, Birnbaum BA.
Thin-section CT imaging of patients suspected of having appendicitis or diverticulitis.
Acad Radiol. 2000 Jan;7(1):48-60. Review. PMID: 10645459
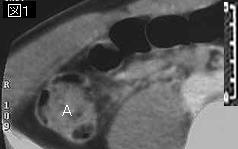
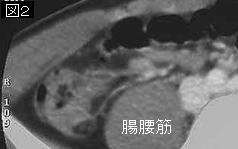
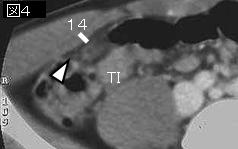
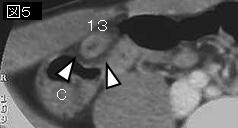
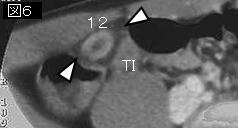
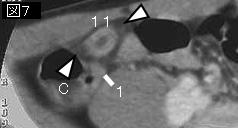
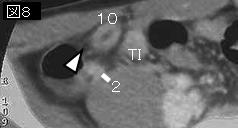
Normal appendix is identified in approximately 44-51 % of routine abdominal CT studies in asymptomatic adults. It arises 2-3 cm caudal to the ileocecal valve from the medial aspect of the cecum and ranges from 2 to 20 cm in length.
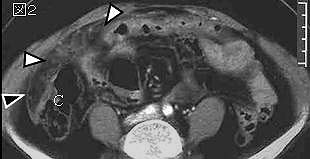
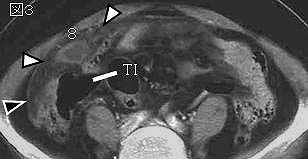
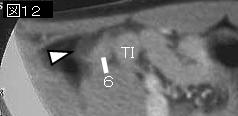
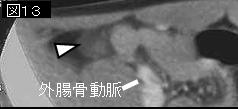
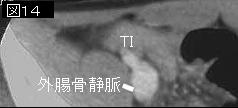
It most commonly appears as a small tubular or ring-like pericecal structure within the right lower quadrant. The appendix is considered normal when the wall is paper-thin, does not enhance with the administration of intravenous contrast medium, and is surrounded by the homogenous density of the normal mesenteric fat. The collapsed appendix should not measure more than 6 mm in diameter. If a calcified appendicolith is identified, it is not considered clinically important unless there are other signs suggesting appendicitis.
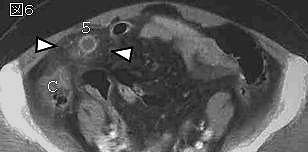
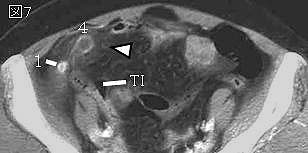
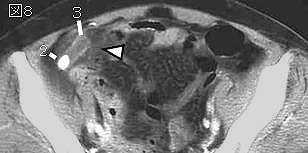
CT findings of acute appendicitis; In mild appendicitis, the inflamed appendix appears as a slightly distended fluid-filled tubular structure that usually measures between 5 and 15 mm in diameter. The appendeceal wall appears circumferentially and symmetrically thickened. The thickened wall is usually homogenously dense on contrast-enhanced studies, a double−halo or target sign may be seen. Periappendiceal inflammation is usually present but may be absent in the most incipient cases. The inflammatory response ranges from subtle clouding of the mesoappendix in patients with mild appendicitis to phlegmon and abscess formation with associated ileocecal thickening in cases of perforation.
A definitive CT diagnosis of appendicitis can be made if an abnormal appendix is identified or if a pericecal abscess or phlegmon is seen in association with appendicolith. The simple presence of pericecal inflammation or an RLQ abscess is suggestive of but not specific for appendicitis.
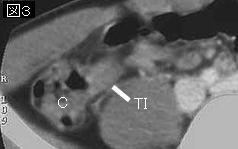
Authors strongly advocate the use of both oral and intravenous contrast media for CT evaluation of the appendix because enhancement of the thickened appendiceal wall enables detection of mild inflammation in incipient cases, aids in identification of the appendix in thin patients with minimal mesenteric fat, and helps distinguish perforated appendicitis from nonspecific pericecal inflammation or abscess in more advanced cases. Intravenous contrast medium is also invaluable in characterizing nonappendiceal gastrointestinal, genitourinary, and gynecologic disease. It is particularly helpful in distinguishing benign from malignant bowel wall thickening, because the presence of mural stratification, or target-sign pattern of enhancement, indicates nonneoplasmic bowel thickening when seen in the small and large bowel. In addition, mesenteric adenopathy can more readily be differentiated from unopacified mesenteric veins after infusion of intravenous contrast material. The use of oral water-soluble iodinated contrast material improves recognition of the normal or abnormal appendix and specifically ileal loops as the appendix.
文献考察2):急性虫垂炎のCT診断
【小児虫垂炎 診断・治療の現況】 小児急性虫垂炎のCT診断(原著論文/特集)
Author:木村賢哉(中京病院(社保)), 松田眞佐男, 弥政晋輔
Source:小児外科(0385-6313)33巻5号 Page480-486(2001.05)
Abstract:臨床所見上急性虫垂炎が疑われた小児63例にCTを施行し検討した.41例で虫垂が描出され,このうち39例を蜂窩織炎性以上の急性虫垂炎と診断し手術を行った.虫垂の最大径はカタル性3例ではいずれも8mm未満であり,蜂窩織炎性23例,壊疽性7例,穿孔性8例では全例で8mm以上であった.急性虫垂炎の手術適応決定におけるCT診断能はsensitivity 100%であった.この結果より,CTを併用する事により診断能が向上した.手術適応の診断基準として,最大径8mm以上の腫大虫垂の描出,虫垂内糞石の存在,虫垂の腫大とともに虫垂および腸管周囲の腹水・膿瘍または周囲脂肪織の濃度上昇が存在する事が妥当であると考えられた.
|