|
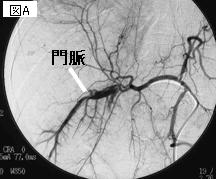
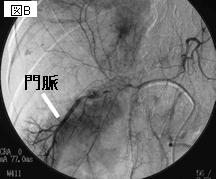
文献考察:arterioportal fistula
1)Gastroenterology. 1997 Oct;113(4):1390-401.
The arterioportal fistula syndrome: clinicopathologic features, diagnosis, and therapy.
Vauthey JN, Tomczak RJ, Helmberger T, Gertsch P, Forsmark C, Caridi J, Reed A, Langham MR Jr, Lauwers GY, Goffette P, Lerut J.
BACKGROUND & AIMS: Arterioportal fistulas (APFs) are rare vascular disorders of the mesenteric circulation. The aim of this study was to determine the etiology, anatomical location, and main symptom at presentation of APFs, and analyze the various modes of treatment. METHODS: The etiology, clinical presentation, radiographs, and treatment of 12 patients with APFs are reported in detail, and another 76 cases published since 1980 are reviewed. RESULTS: APFs result from trauma (n = 25, 28%), iatrogenic procedures (n = 14, 16%), congenital vascular malformations (n = 13, 15%), tumor (n = 13, 15%), aneurysm (n = 12, 14%), and other causes (n = 11, 12%). The origin of APFs is the hepatic artery in the majority of patients (n = 56, 65%). The main symptoms at presentation are lower or upper gastrointestinal bleeding (n = 29, 33%), ascites (n = 23, 26%), heart failure (n = 4.5%), or diarrhea (n = 4.5%). Radiological intervention provides definitive treatment in 42% (n = 33) of patients, whereas the remainder are treated by surgery alone (n = 27, 31%) or a combination of radiological intervention and surgery (n = 8, 9%). CONCLUSIONS: APFs result in a protean syndrome variously combining portal hypertension and other hemodynamic imbalances (heart failure, intestinal ischemia). Single or multiple interventional radiological procedures using arterial and/or venous approaches allow definitive treatment of most APFs. With increasing technological advances, it is anticipated that surgery will only be indicated in rare instances after failure of radiological intervention(s).PMID: 9322535
2)Korean J Radiol. 2002 Jan-Mar;3(1):1-15.
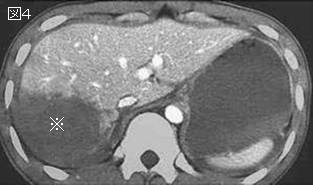
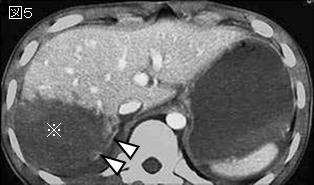
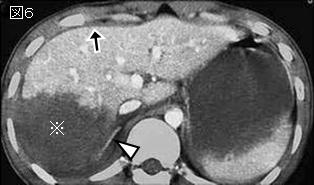
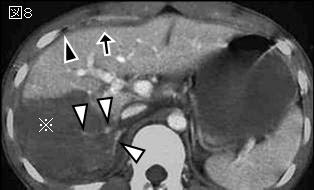
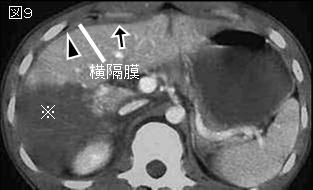
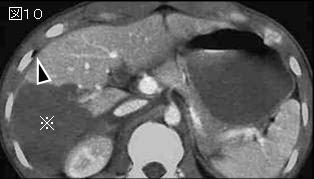
Hepatic arterioportal shunts: dynamic CT and MR features.
Choi BI, Lee KH, Han JK, Lee JM.
With the increased temporal resolution available in dynamic computed tomography (CT) and magnetic resonance imaging (MRI), hepatic arterioportal shunts are now more frequently encountered than in the past. The condition occurs in various hepatic diseases in which portal or hepatic venous flow is compromised. The underlying mechanism and the degree of shunt affect its appearance at dynamic imaging. The dynamic CT and MRI findings have been summarized as early enhancement of peripheral portal veins, and wedge-shaped transient parenchymal enhancement during the hepatic arterial phase. Recognition of arterioportal shunt can suggest the presence of a previously unsuspected disorder and avoids false-positive diagnosis or overestimation of a hepatic disease. Familiarity with the pathophysiology of arterioportal shunt also allows investigation of the hepatic hemodynamic changes occurring in various hepatic diseases.PMID: 11919473
|