|
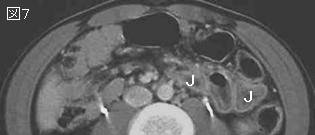
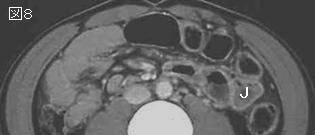
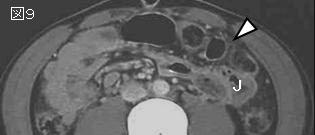
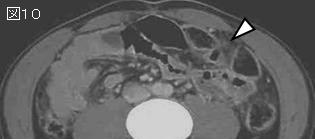
文献考察:鈍的外傷による小腸穿孔は受傷後8時間を過ぎると死亡率と術後合併症が急増する.
J Trauma. 2000 Mar;48(3):408-14; discussion 414-5.
Relatively short diagnostic delays (.
Fakhry SM, Brownstein M, Watts DD, Baker CC, Oller D.
OBJECTIVE: Blunt small bowel injury (SBI) is uncommon, and its timely diagnosis may be difficult. The impact of operative delays on morbidity and mortality has been unclear. The purpose of this study was to determine the relationship of diagnostic delays to morbidity and mortality in blunt SBI. METHODS: Patients with blunt SBI with perforation were identified from the registries of eight trauma centers (1989-1997). Patients with duodenal injuries were excluded. Data were extracted by individual chart review. Patients were classified as multi-trauma (group 1) or near-isolated SBI (group 2 with Abbreviated Injury Scale score within 8 hours: 2%; 8-16 hours: 9.1%; 16-24 hours: 16.7%; greater than 24 hours: 30.8%, p = 0.009) as did the incidence of complications. Delays as short as 8 hours 5 minutes and 11 hours 15 minutes were associated with mortality attributable to SBI. The rates of delay in diagnosis were not significantly associated with age, gender, intoxication, transfer status, or presence of associated injuries. CONCLUSION: Delays in the diagnosis of SBI are directly responsible for almost half the deaths in this series. Even relatively brief delays (as little as 8 hours) result in morbidity and mortality directly attributable to "missed" SBI. Further investigation into the prompt diagnosis of this injury is needed. PMID: 10744277
|