|
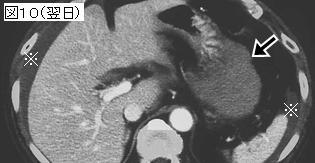
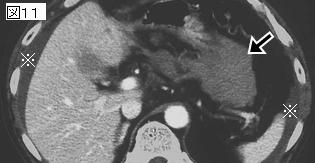
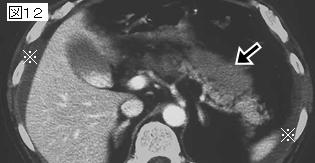
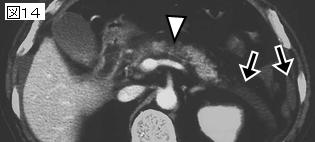
文献考察:膵管損傷を伴う膵損傷に対するステント治療
J Pediatr Surg. 2001 Feb;36(2):345-8.
Treatment of pancreatic duct disruption in children by an endoscopically placed stent.
Canty TG Sr, Weinman D.
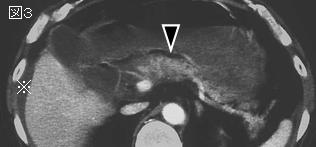
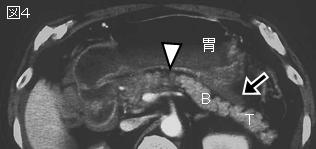
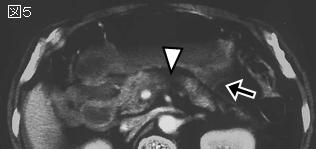
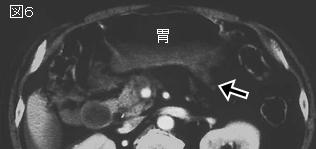
BACKGROUND: Injuries to the pancreas from blunt abdominal trauma in children are rare. Most are minor and are best treated conservatively. The mainstay for treatment of major ductal injuries has been prompt surgical resection. Diagnostic imaging modalities are the key to the accurate classification of these injuries and planning appropriate treatment. Computed tomography (CT) scan has been the major imaging modality in blunt abdominal trauma for children, but has shortcomings in the diagnosis of pancreatic ductal injury. Endoscopic retrograde cholangiopancreatography (ERCP) has been shown recently to be superior in diagnostic accuracy. The therapeutic placement of stents in the trauma setting has not been described in children. METHODS: Two children sustained major ductal injuries from blunt abdominal trauma that were suspected, but not conclusively noted, on initial CT scan. Both underwent ERCP within hours of injury. In case 1, a stent was threaded through the disruption into the distal duct. In case 2, a similar injury, the stent could only be placed through the ampulla, thereby reducing ductal pressure. In both cases, clinical improvement was rapid with complete resolution of clinical and chemical pancreatitis, resumption of a normal diet, and discharge from the hospital. The stents were removed at 10 and 12 days postinjury, and both children have remained well. Follow-up ERCP and CT scans show complete healing of the ducts and no evidence of pseudocyst formation 1 year post injury. CONCLUSIONS: Acute ERCP should be the imaging modality of choice in suspected major pancreatic ductal injury. Successful treatment by placement of an intrapancreatic ductal stent may be possible at the same time. Surgical resection or reconstruction can then be reserved for cases in which stenting is impossible or fails.PMID: 11172431
追記:上記症例のような”side hole injury”(膵管の部分断裂)2例に膵管にステントを留置し,治療に成功した.
|