|
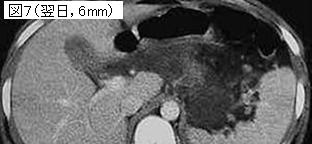
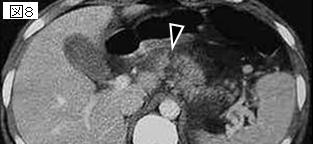
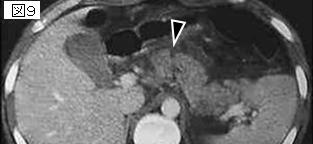
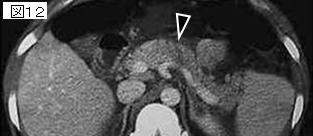
文献考察:膵損傷のCT所見・膵損傷の診断率を向上するには
JBR-BTR. 2000 Aug;83(4):160-6.
Diagnosis of pancreatic injury: a need to improve performance.
Dondelinger RF, Boverie JH, Cornet O.
A direct frontal upper abdominal impact and a bicycle fall in a child are classical mechanisms of blunt pancreatic injury. Clinical symptoms are not characteristic. Serum amylase level is frequently normal at admission and peritoneal lavage fluid amylase is not diagnostic. CT is the most powerful imaging technique to evidence pancreatic contusion and associated injuries but remains normal or doubtful at admission in about 15% of children and 40% of adults. US is sensitive in about 70%. Both modalities are unable to detect pancreatic duct rupture. As ERP cannot be performed in all trauma patients, only patients with minor pancreatic injury can be enrolled in a conservative management without surgical revision. The role of multislice CT at admission and MRP has to be investigated to increase diagnostic efficiency in pancreatic duct injury.Review PMID: 11126785
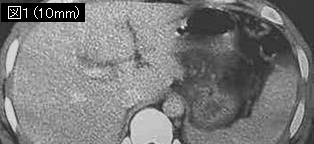
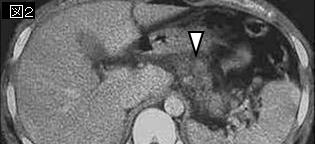
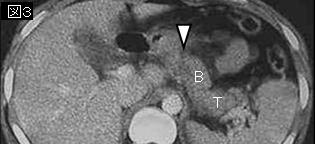
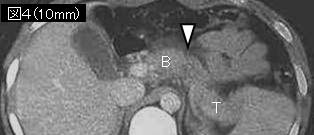
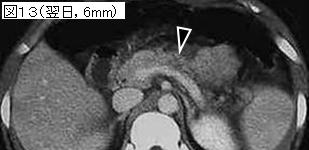
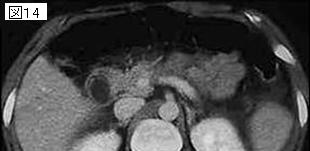
追記:膵損傷のCT所見.1:膵実質内の境界不鮮明な低吸収域,2:正常に造影される膵実質を分断する断裂像,3:部分的なまたはびまん性の膵腫大,4:膵周囲(後腹膜)の液貯留または血腫,5:腹腔内腹水,6:十二指腸損傷所見.確定診断に至らず,しかし疑わしければ12〜24時間内に4〜5mmスライスCTを再撮影すべき.
|