|
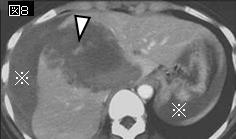
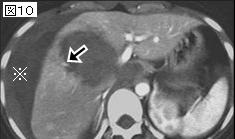
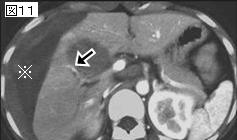
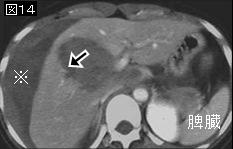
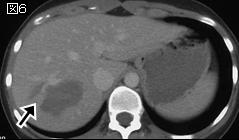
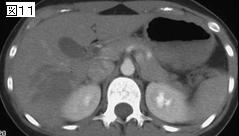
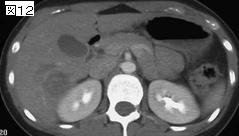
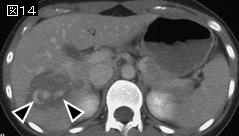
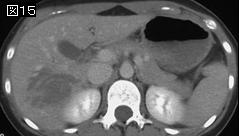
文献考察:TAEは極めて有効な治療法だが,AAST Grade IVとVで,血圧を維持するのに2000ml以上の輸液を必要な症例は手術の適応
1)J Trauma. 2002 Jun;52(6):1091-6.
The efficacy and limitations of transarterial embolization for severe hepatic injury.
Hagiwara A, Murata A, Matsuda T, Matsuda H, Shimazaki S.
Department of Traumatology and Critical Care Medicine, Kyorin University, School of Medicine, Tokyo, Japan.
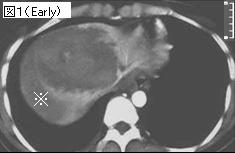
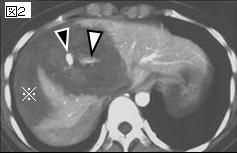
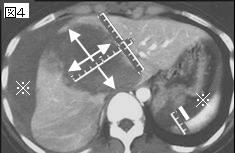
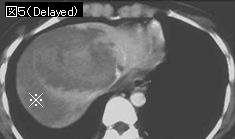
BACKGROUND: The efficacy of transarterial embolization (TAE) for severe blunt hepatic injury has been reported. We performed a prospective study evaluating the efficacy and the limitation of TAE from January 1996 to December 2000. METHODS: All patients with blunt abdominal injury who could be stabilized by fluid resuscitation underwent computed tomographic (CT) scan examinations. Patients with CT scan evidence of hepatic injury were classified into five grades according to CT scan findings on the basis of the injury scale of the American Association for the Surgery of Trauma (Mirvis classification). All patients with CT scan grade 3 to 5 injury underwent angiography. When angiography showed extravasation of contrast medium extending from hepatic arterial branches, TAE was performed. RESULTS: Of 612 patients with blunt abdominal trauma, 51 had CT scan grade 3 to 5 injury. Thirty-seven of these patients had a CT scan grade 3 injury and 18 underwent TAE. One of 19 patients who did not undergo TAE developed a delayed hemorrhage on day 6 and required a laparotomy. All 13 patients with a CT scan grade 4 injury had angiographic findings of the extravasation. TAE was successful in 11 patients and unsuccessful in 2. Five patients with a CT scan grade 4 injury required laparotomy. One developed a delayed hemorrhage on day 4. The remaining four patients had a major venous injury (a right lobectomy was performed in two with inferior vena cava injury, and a gauze packing in two with hepatic venous injury). One patient with a CT scan grade 5 injury underwent immediate laparotomy after TAE. Laparotomy revealed inferior vena cava injury and a right lobectomy was performed. Only two patients who underwent a lobectomy died of an uncontrollable hemorrhage. All CT scans of patients with hepatic venous or inferior vena cava injury showed a large low-density area (> or = 10 cm) with involvement of these vessels. The volumes of fluid resuscitation needed from admission until TAE ranged from 2,109 to 2,638 mL/h. CONCLUSION: It was considered that the combination of the presence of a CT scan grade 4 or 5 lesion and the fluid requirements of more than 2,000 mL/h to maintain normotension indicated the absolute necessity of surgery. We felt that these patients were not candidates for TAE, and should undergo immediate laparotomy. PMID: 12045635
2)J Trauma. 2004 Aug;57(2):271-6; discussion 276-7.
The usefulness of transcatheter arterial embolization for patients with blunt polytrauma showing transient response to fluid resuscitation.
Hagiwara A, Murata A, Matsuda T, Matsuda H, Shimazaki S.
Department of Traumatology and Critical Care Medicine, School of Medicine, Kyorin University, Tokyo, Japan. hagiwarapupu@jcom.home.ne.jp
BACKGROUND: This study aimed to determine whether nonsurgical management using transcatheter arterial embolization (TAE) is safe for patients with blunt multiple trauma who transiently respond to the initial fluid resuscitation. METHODS: Contrast computed tomography was performed for patients with blunt abdominal injuries, excluding those who did not respond to initial fluid resuscitation. Angiography was performed for patients with injuries showing contrast extravasation or solid organ injury classified, according to the American Association for the Surgery of Trauma, as grade 3 or higher on computed tomography. Transcatheter arterial embolization was performed when angiography showed arterial extravasation. The protocol was abandoned for any patients who became profoundly hypotensive (with systolic blood pressure 60 mm Hg or lower) during computed tomography or angiography. RESULTS: Between January 2000 and December 2002, 269 patients with blunt abdominal injuries underwent TAE immediately after admission. Of these patients, 41 had injuries in at least two regions and underwent TAE for these regions. Among them, 22 patients were hemodynamically stable or showed rapid response to fluid resuscitation. The nonsurgical treatment was successful in all these cases. The remaining 19 patients (Injury Severity Score, 37.3 +/- 8.2), who showed a transient response, were the subjects of this study. Of these patients, 15 underwent TAE for injuries in two regions (13 pelvic fractures, 7 splenic injuries, 6 hepatic injuries, 3 facial bleeding, and 1 renal injury), and 4 patients underwent TAE for injuries in three regions (4 had splenic injuries, 3 hepatic injuries, 2 renal injuries, 2 pelvic fractures, and 1 facial bleeding). For all these patients, TAE was successfully performed. Before TAE, the systolic blood pressure was 79.9 +/- 8.4 mm Hg, and the shock index was 1.45 +/- 0.25 mm Hg. After TAE, the corresponding values were 120.6 +/- 19.3 mm Hg and 0.87 +/- 0.16 mm Hg, respectively (p
追記:低血圧を呈する症例は,一般的には血管造影よりも手術の適応であるが,初期輸液2000mlで血圧の改善が認められるならTAEを施行して保存的治療が可能である
|