|
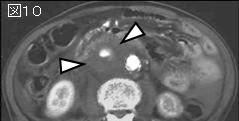
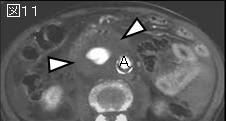
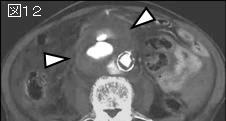
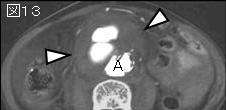
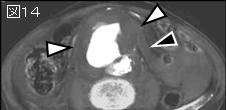
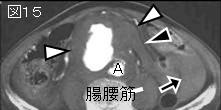
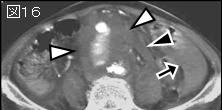
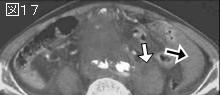
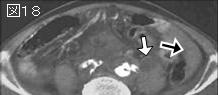
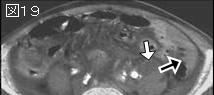
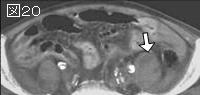
文献考察:感染性腹部大動脈瘤.全胸腹部および腸骨動脈瘤中感染性は1.3%.発熱があったのは48%,24%は既に穿孔していた.死亡率は36%.
1)J Vasc Surg. 2001 Jan;33(1):106-13.
Mycotic aneurysms of the thoracic and abdominal aorta and iliac arteries: experience with anatomic and extra-anatomic repair in 33 cases.
Muller BT, Wegener OR, Grabitz K, Pillny M, Thomas L, Sandmann W.
OBJECTIVE: A mycotic aneurysm of the aorta and adjacent arteries is a dreadful condition, threatening life, organs, and limbs. With regard to the aortic segment involved, repair by either in situ replacement or extra-anatomic reconstruction can be quite challenging. Even when surgery has been successful, the prognosis is described as very poor because of the weakened health status of the patient who has developed this type of aneurysm. The aim of our study was to find out whether any progress could be achieved in a single center over a long time period (18 years) through use of surgical techniques and antiseptic adjuncts. MATERIAL AND METHODS: From January 1983 to December 1999, a total of 2520 patients with aneurysms of the thoracic and abdominal aorta and iliac arteries underwent surgery for aortic or iliac replacement at our institution. During that period, 33 (1.31%) of these patients (mean age, 64.3 years) were treated for mycotic aneurysms of the lower descending and thoracoabdominal (n = 13), suprarenal (n = 4), and infrarenal (n = 10) aorta and iliac arteries (n = 6). Twenty (61%) of these 33 patients had histories of various septic diseases; in the other 13 (39%), the etiology remained uncertain. Preoperative signs of infection, such as leukocytosis and elevated C-reactive protein, were found in 79% of the patients, and fever was apparent in 48%; 76% of the patients complained of pain. At the time of surgery, eight (24%) mycotic aneurysms were already ruptured, and 20 (61%) had penetrated into the periaortic tissues, forming a contained rupture. Five (15%) aneurysms were completely intact. The predominant microorganisms found in the aneurysm sac were Staphylococcus aureus and Salmonella species. Careful debridement of all infected tissue was essential. In the infrarenal aortic and iliac vascular bed, in situ reconstruction was performed only in cases of anticipated "low-grade" infection. Alternative revascularization with extra-anatomic procedures (axillobifemoral or femorofemoral crossover bypass graft) was carried out in eight of 16 cases. All four suprarenal and all 13 mycotic aneurysms of the thoracoabdominal aortic segment were repaired in situ. Antibiotics were administered perioperatively, and all patients were subsequently treated with long-term antibiotics. RESULTS: In-hospital mortality was 36% (n = 12). Because of the smallness and heterogeneity of the sample, we could not demonstrate significant evidence for any influence of aneurysm location or type of reconstruction on patients' outcome. However, survival was clearly influenced by the status of rupture. During long-term follow-up (mean, 30 months; range, 1-139 months), 10 patients (48%) died-one (4.8%) probably as a consequence of the mycotic aneurysm, the others for unrelated reasons. Eleven patients (52%) are alive and well today, with no signs of persistent or recurrent infection. CONCLUSIONS: A mycotic aneurysm of the aortic iliac region remains a life-threatening condition, especially if the aneurysm has already ruptured by the time of surgery. Although the content of the aneurysm sac is considered septic, as was proved by positive cultures in 85% of our patients, in situ reconstruction is feasible and, surprisingly, was not more closely related to higher morbidity and mortality in our series than ligation and extra-anatomic reconstruction, although most of the aneurysms repaired in situ were located at the suprarenal and thoracoabdominal aorta. We assume that our operative mortality rate of 36%, which relates to a rupture rate of 85%, could be substantially lowered if the diagnosis of mycotic aneurysm were established before rupture. PMID: 11137930
2)死亡率が高いrisk factorは高齢者,サルモネラ菌以外の起炎菌,非手術例.
J Vasc Surg. 2004 Jul;40(1):30-5.
Infected aortic aneurysms: clinical outcome and risk factor analysis.
Hsu RB, Chen RJ, Wang SS, Chu SH.
PURPOSE: Infected aortic aneurysms are difficult to treat, and are associated with significant mortality. Hospital survival is poor in patients with severe aortic infection, Salmonella species infection, Staphylococcus aureus infection, aneurysm rupture, and suprarenal aneurysm location. We reviewed the clinical outcome in 46 patients with primary infected aortic aneurysms and identified clinical variables associated with prognosis. METHODS: Data were collected by means of retrospective chart review. Univariate and multivariate logistic regression models were used for risk factor analysis. RESULTS: Between August 1995 and March 2003, 48 patients with primary infected aortic aneurysms were treated at our hospitals. Two patients with negative culture results were excluded. Of the remaining 46 patients, 35 patients had aortic aneurysms infected with Salmonella species and 11 patients had aortic aneurysms infected with microorganisms other than Salmonella species. There were 20 suprarenal infections and 26 infrarenal infections. Surgical debridement and in situ graft replacement were performed in 35 patients, with an early mortality rate of 11%. The incidence of late prosthetic graft infection was 10%. The 90-day mortality rate in patients operated on was 0% for elective operation and 36% for nonelective operation (P =.006, Fisher exact test). Independent predictors of aneurysm-related death were advanced age, non-Salmonella infection, and no operation. CONCLUSION: With timely surgical intervention and prolonged antibiotic treatment, in situ graft replacement provides an excellent outcome in patients with primary infected aortic aneurysms and elective operation. Mortality is still high in patients undergoing urgent operation. Advanced age, non-Salmonella infection, and no operation are major determinants of mortality. PMID: 15218459
3)腸腰筋膿瘍を合併した破裂性感染性腹部大動脈瘤の1例 感染経路・術式の一考察
Author:一和多雅雄(東十条病院), 新野成隆, 前田英明, 瀬在明, 根岸七雄, 瀬在幸安
Source:日本血管外科学会雑誌(0918-6778)8巻5号 Page601-606(1999.08)
要旨:今回われわれは,腸腰筋膿瘍を合併した破裂性感染性腹部大動脈瘤を経験した.動脈瘤組織および腸腰筋内容物を十分にデブリードメント・洗浄を行い,非解剖学的経路による血行再建を行った.術中に採取した膿汁よりstreptococcus sp.が検出され,術後に感染のコントロールがつかず,敗血症を合併し第73病日に死亡した.
1998年10月までに感染性腹部大動脈瘤(以下IAAA)は世界で268例が報告されており,特異的感染を除いた本邦での報告例は48例である.268例中,腸腰筋膿瘍を合併したIAAAは,自験例を含めて15例(5.5%)であった.15例を検討すると男性14例,女性1例と圧倒的に男性が多く,平均年齢は61.5±9・4歳であった.起因菌は11例/15例(73%)がsalmonella属であり,グラム陰性桿菌が14例/15例(93%)を占めていた.腸腰筋膿瘍を合併したIAAAの感染経路としては,1)IAAAから腸腰筋に感染が波及した場合,2)消化管などの遠隔臓器からの2次性腸腰筋膿瘍が発症しIAAAの発症に起因する場合,の2経路が考えられた.術式の選択としては非解剖学的血行再建を第1選択とすべきであると思われる.
|