|
参考文献
1)Medicine (Baltimore). 1999 Nov;78(6):386-94.
Acute renal infarction. Clinical characteristics of 17 patients.
Domanovits H, Paulis M, Nikfardjam M, Meron G, Kurkciyan I, Bankier AA, Laggner AN.
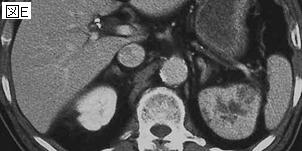
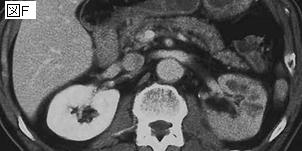
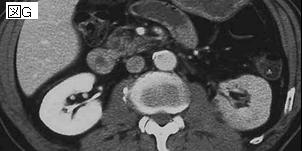
We analyzed the medical records of patients with an established diagnosis of acute renal infarction to identify predictive parameters of this rare disease. Seventeen patients (8 male) who were admitted to our emergency department between May 1994 and January 1998 were diagnosed by contrast-enhanced computed tomography (CT) as having acute renal infarction (0.007% of all patients). We screened the records of the 17 patients for a history with increased risk for thromboembolism, clinical symptoms, and urine and blood laboratory results known to be associated with acute renal infarction. A history with increased risk for thromboembolism with 1 or more risk factors was found in 14 of 17 patients (82%); risk factors were atrial fibrillation (n = 11), previous embolism (n = 6), mitral stenosis (n = 6), hypertension (n = 9), and ischemic cardiac disease (n = 7). All patients reported persisting pain predominantly from the flank (n = 11), abdomen (n = 4), and lower back (n = 2). On admission, elevated serum lactate dehydrogenase was found in 16 (94%) patients, and hematuria was found in 12 (71%) of 17 patients. After 24 hours all patients showed an elevated serum lactate dehydrogenase, and 14 (82%) had a positive test for hematuria. Our findings suggest that in all patients presenting with the triad--high risk of a thromboembolic event, persisting flank/abdominal/lower back pain, elevated serum levels of lactate dehydrogenase and/or hematuria within 24 hours after pain onset--contrast-enhanced CT should be performed as soon as possible to rule out or to prove acute renal infarction. PMID: 10575421
2)Eur Urol. 2000 Sep;38(3):339-43.
Local thrombolytic treatment for renal arterial embolism.
Gluck G, Croitoru M, Deleanu D, Platon P.
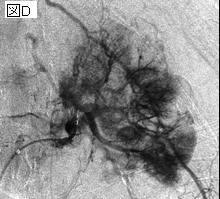
OBJECTIVE: To determine the utility of local thrombolysis in the treatment of acute renal arterial occlusion. METHODS: We used local thrombolytic treatment in a female patient, aged 76, with 72 h of anuria, right lumbar and flank pain. She had a 3-year history of ischemic heart disease and atrial fibrillation controlled with digital treatment. Also, she was nephrectomized on the left side 33 years ago for lithiasic pyonephrosis. A normal right urinary tract was demonstrated with ultrasound examination, KUB radiography and retrograde pyelography. The next step was diagnostic abdominal angiography and local thrombolytic treatment with streptokinase. RESULT: Thrombolysis with streptokinase was successful following 72 h of renal artery occlusion. After 24 months the patient is doing well. CONCLUSION: Local intra-arterial thrombolysis is the treatment of choice in renal artery occlusion. PMID: 10940710
|