|
文献考察:Ogilvie症候群
Curr Treat Options Gastroenterol. 2000 Aug;3(4):273-286.
Acute Intestinal Pseudo-obstruction.
Quigley EM.
Acute pseudo-obstruction may manifest clinically in one of three forms--acute gastroparesis, ileus, and acute colonic pseudo-obstruction (Ogilvie's syndrome). Though formerly associated primarily with the postoperative state, these entities are increasingly recognized in association with a wide variety of major medical problems. There are few controlled studies to guide the clinician in the management of these disorders. Treatment remains largely empirical, and time-honored, based primarily on "bowel rest," nasogastric decompression, and supportive care. While a wide variety of pharmacologic approaches have been advocated, few have been subjected to, or survived, the rigors of a properly controlled trial. Neostigmine is a notable exception, and has been shown to be effective in Ogilvie's syndrome. Perforation is a significant threat in megacolon; colonoscopic, or surgical decompression may, therefore, be indicated. Both are associated with significant risks in this context, but may prevent progression to perforation with its attendant mortality. New approaches seek to exploit current concepts in the pathophysiology of ileus and megacolon but have not, as yet, achieved efficacy in human studies. PMID: 11096588
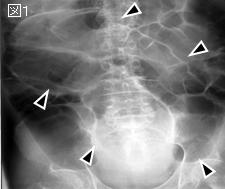
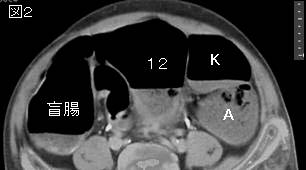
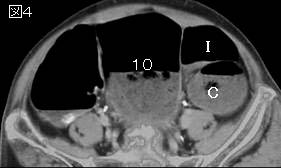
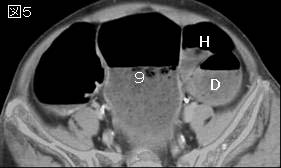
追記:大腸穿孔の頻度は3%.盲腸は直径9cmから異常であるが,12cmを超えると穿孔のリスクは高い.盲腸の拡張が6日以上経過すると穿孔の危険が増す.Neostigmine2mg静注が効果的なことがある.
|