|
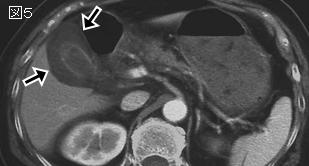
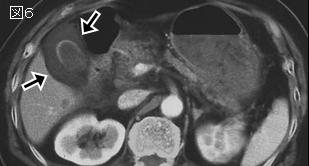
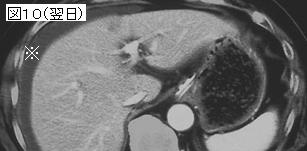
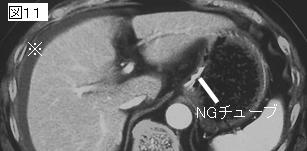
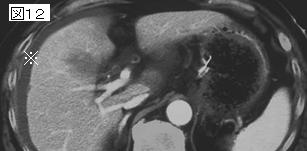
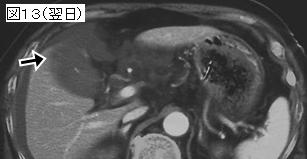
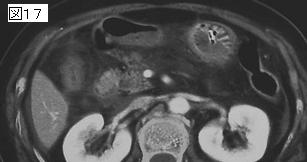
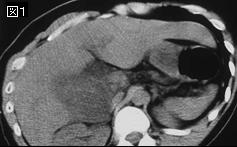
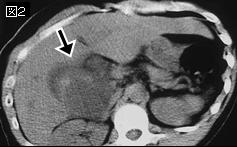
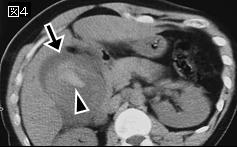
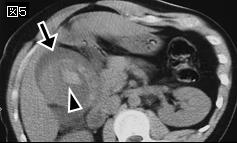
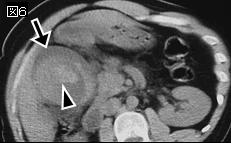
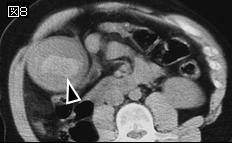
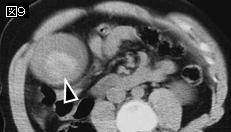
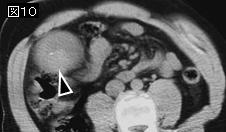
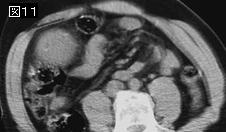
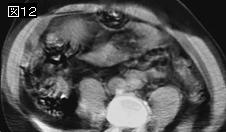
文献考察1):胆嚢損傷のCT所見(表1)
Radiographics. 2004 Sep-Oct;24(5):1381-95.
Blunt trauma of the pancreas and biliary tract: a multimodality imaging approach to diagnosis.
Gupta A, Stuhlfaut JW, Fleming KW, Lucey BC, Soto JA.
Injuries of the pancreas, gallbladder, and bile ducts due to blunt trauma are relatively uncommon and difficult to detect but are associated with high morbidity and mortality, especially if diagnosis is delayed. Accurate and early diagnosis is imperative, and imaging plays a key role in detection. Knowledge of the mechanisms of injury, the types of injuries, and the roles of various imaging modalities is essential for prompt and accurate diagnosis. Early recognition of disruption of the main pancreatic duct is important because such disruption is the principal cause of delayed complications. Computed tomography (CT) can demonstrate pancreatic parenchymal injuries and complications such as abscess, fistula, pancreatitis, and pseudocyst. CT findings can also suggest disruption of the pancreatic duct; however, the ability of CT to indicate this finding depends on the degree of parenchymal injury. Magnetic resonance (MR) cholangiopancreatography allows direct imaging of the pancreatic duct and sites of disruption. Gallbladder injuries can be detected with CT, ultrasonography, hepatobiliary scintigraphy, or MR cholangiopancreatography. CT findings include a collapsed gallbladder, wall thickening, inhomogeneous mural enhancement, and pericholecystic fluid. Bile duct injuries can be suggested with CT, which may show ascites and associated liver injuries, and can be confirmed with hepatobiliary scintigraphy. PMID: 15371615(full text)
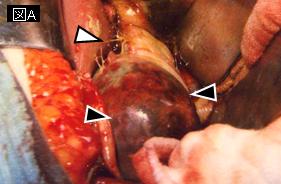
文献考察2):170例の検討(表2)
J Trauma. 1995 Sep;39(3):576-80.
Blunt gallbladder injuries: presentation of twenty-two cases with review of the literature.
Sharma O.
Blunt injuries to the gallbladder are very uncommon, whereas penetrating gallbladder trauma occurs more frequently. Over the last 19-year period through 1994, 22 cases with blunt gallbladder trauma were treated. Avulsion (partial or complete) and contusion were observed in 10 cases each (45%). Perforation of the gallbladder and traumatic cholecystitis with necrosis were seen in one case each. Associated intra-abdominal trauma was present in 100% of the cases and accounted for both mortalities. Gallbladder injury was diagnosed after celiotomy, except for one case that was diagnosed and treated nonoperatively. Based on the experiences gained herein and an extensive review of the literature, a classification scheme for gallbladder trauma and its treatment is presented.PMID: 7473927
|









;){kind=link}
;){kind=link}