|
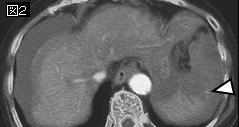
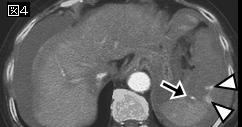
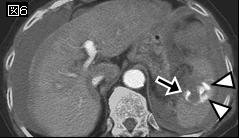
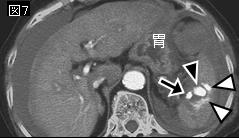
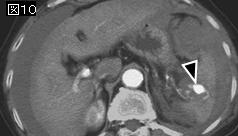
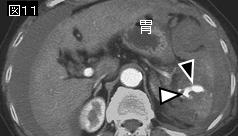
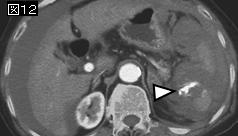
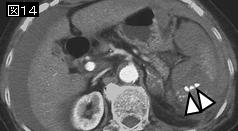
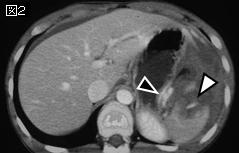
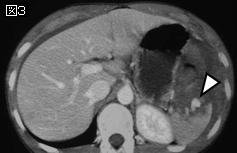
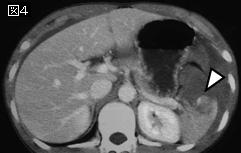
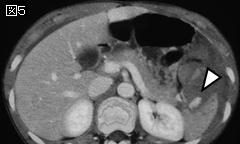
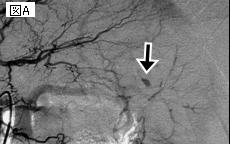
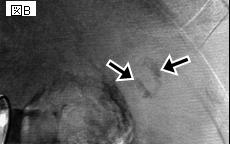
文献考察:脾臓外傷のAAST分類ではextravasationや仮性動脈瘤の所見が考慮されていない.新分類は血管造影または手術を要する症例の選択により正確である(表1,2,3).
AJR Am J Roentgenol. 2007 Dec;189(6):1421-7.
Optimization of selection for nonoperative management of blunt splenic injury: comparison of MDCT grading systems.
Marmery H, Shanmuganathan K, Alexander MT, Mirvis SE.
OBJECTIVE: The purpose of this study was to compare the usefulness of two CT grading systems of blunt splenic trauma in predicting which patients need surgery or angioembolization. MATERIALS AND METHODS: Four hundred patients in hemodynamically stable condition admitted with blunt splenic injury were included in the study. All patients underwent contrast-enhanced MDCT. Grade of splenic injury was prospectively assigned according to the American Association for the Surgery of Trauma (AAST) splenic injury scale. Patients were treated with surgical intervention, splenic arteriography with or without embolization, or observation alone. All MDCT images were retrospectively reviewed and regraded according to a novel grading system that specifically incorporates the findings of active bleeding or splenic vascular injury, including pseudoaneurysm and arteriovenous fistula. Receiver operating characteristics curves were generated with both grading systems for all splenic interventions, and statistical analyses were performed. RESULTS: The area under the ROC curves for the new splenic grading system for splenic arteriography, surgery, and both interventions exceeded 80%. The area under the curve for the new splenic grading system was greater than that for the AAST injury scale for all interventions. Differences were found to be statistically significant for splenic arteriography (p = 0.0036) and the combination of arteriography and surgery (p = 0.0006). CONCLUSION: The proposed CT grading system is better than the AAST system for predicting which patients with blunt splenic trauma need arteriography or splenic intervention.PMID: 18029880(full text)
|














;){kind=link}
;){kind=link}
;){kind=link}