|
文献考察:seat belt sign
1)Radiographics. 1991 Jan;11(1):23-36. (表1,表2)
Seat belt injuries: radiologic findings and clinical correlation.
Hayes CW, Conway WF, Walsh JW, Coppage L, Gervin AS.
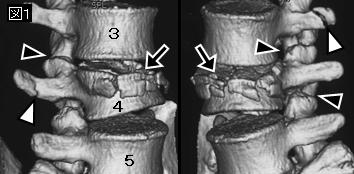
The seat belt syndrome consists of skeletal, soft-tissue, and visceral injuries associated with use of two- and three-point restraints in patients involved in motor vehicle accidents. Skin abrasions of the neck, chest, and abdomen--the classic seat belt sign--indicate internal injury in 30% of cases. Neck abrasions are associated with injuries to the carotid artery, larynx, and cervical spine; chest abrasions, with fractures of the sternum, ribs, and clavicles and injuries to the heart and thoracic aorta; and abdominal abrasions, with mesenteric tears, bowel perforation and hematoma, Chance fractures, and injuries to the abdominal aorta. The seat belt sign should prompt a diligent search for related injuries.PMID: 1996397(full text)
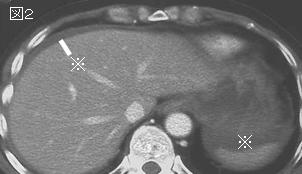
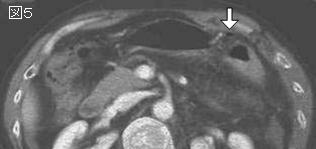
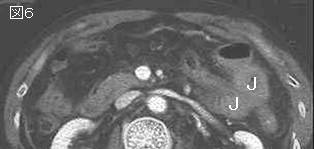
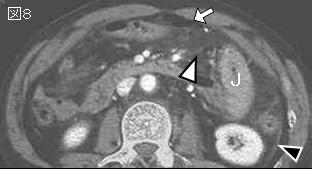
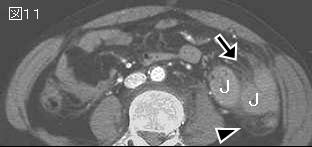
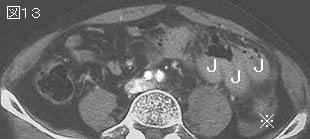
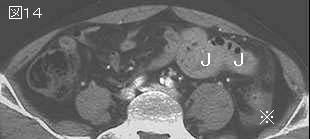
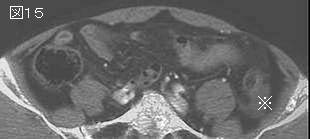
2)seat belt signを有する23例の腹部外傷は,小腸穿孔78%,大腸穿孔30%,腸管漿膜損傷35%,腸間膜22%,70%が多発外傷.FASTによる診断率は低い.
Arch Surg. 2002 Jun;137(6):718-22; discussion 722-3.
Abdominal seat belt marks in the era of focused abdominal sonography for trauma.
Stassen NA, Lukan JK, Carrillo EH, Spain DA, Richardson JD.
HYPOTHESIS: Focused abdominal sonography for trauma (FAST) is an unreliable method for assessing intra-abdominal injury in patients with seat belt marks. DESIGN: Retrospective review of trauma patients with intestinal injury and seat belt marks during a 3-year period. Records were reviewed for patient demographics, FAST results, computed tomographic (CT) scan results, and operative findings. The CT scan results were considered positive if bowel wall thickening, extraluminal air, or free fluid without solid organ injury were present. SETTING: University hospital designated as a level I trauma center. PATIENTS: Twenty-three patients who required operation for intestinal or mesenteric injury and who had an abdominal seat belt mark. MAIN OUTCOME MEASURE: Sensitivity of FAST in these patients. RESULTS: All patients were evaluated using both FAST and CT scan of the abdomen and pelvis. Eighteen patients (78%) had either negative or equivocal FAST results when significant intestinal injury was present. All 23 patients had CT scan findings suggestive of bowel or mesenteric injury. Moderate-to-large free intraperitoneal fluid without solid organ injury was the most common finding (n = 21, 91%). Operative findings included small-bowel perforation (n = 18, 78%), colonic perforation (n = 7, 30%), bowel deserosalization (n = 8, 35%), and isolated mesenteric injury (n = 5, 22%). Sixteen patients (70%) had multiple intra-abdominal injuries. All patients were taken directly from the emergency department to the operating room. Seventeen percent of operative explorations (4/23) were nontherapeutic (no repairs required). CONCLUSION: This study confirms that FAST cannot reliably exclude intestinal injury in patients with seat belt marks.PMID: 12049544(full text)
|









;){kind=link}
;){kind=link}