|
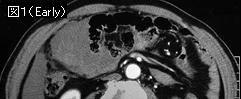
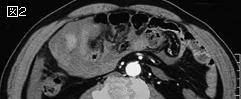
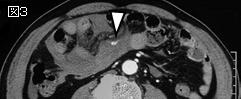
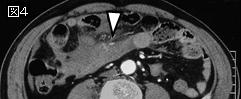
文献考察:腸管および腸間膜損傷のCT所見
1)J Trauma. 2000 Jun;48(6):991-8; discussion 998-1000.
Blunt bowel and mesenteric injuries: the role of screening computed tomography.
Malhotra AK, Fabian TC, Katsis SB, Gavant ML, Croce MA.
BACKGROUND: Early generation scanners have demonstrated poor sensitivity detecting blunt bowel/mesenteric injuries (BBMI). This study was aimed at determining the accuracy and role of helical scanners in BBMI. METHODS: Retrospective chart review of patients with BBMI, or computed tomographic scans suspicious of BBMI, from August of 1995 to December of 1998. RESULTS: One hundred of 8,112 scans (1.2%) were suspicious of BBMI. Of these suspicious scans, 53 patients had BBMI (true positive-TP) and 47 patients did not (false positive-FP). Seven patients with negative scans had BBMI (false negative-FN). Computed tomography contributed toward early surgery in 77% of patients who may have been delayed. Six patients developed intra-abdominal abscess. The abscess group had a significantly longer time interval from injury to surgery. Multiple findings were seen in 57% of true positive scans, whereas in 13% of false positive scans (p
2)Radiographics. 2006 Jul-Aug;26(4):1119-31.
Evaluation of bowel and mesenteric blunt trauma with multidetector CT.
Brofman N, Atri M, Hanson JM, Grinblat L, Chughtai T, Brenneman F.
Bowel and mesenteric injuries are detected in 5% of blunt abdominal trauma patients at laparotomy. Computed tomography (CT) has been shown to be accurate for the diagnosis of bowel and mesenteric injuries and is the diagnostic test of choice in the evaluation of blunt abdominal trauma in hemodynamically stable patients. Specific CT findings of bowel and mesenteric injuries include bowel wall defect, intraperitoneal and mesenteric air, intraperitoneal extraluminal contrast material, extravasation of contrast material from mesenteric vessels, and evidence of bowel infarct. Specific signs of mesenteric injury are vascular beading and abrupt termination of mesenteric vessels. Less specific signs of bowel and mesenteric injuries include focal bowel wall thickening, mesenteric fat stranding with focal fluid and hematoma, and intraperitoneal or retroperitoneal fluid. When only nonspecific signs of bowel and mesenteric injuries are seen on CT images, correlation of CT features with clinical findings is necessary. A repeat CT examination after 6-8 hours if the patient's condition is stable may help determine the significance of these nonspecific findings. PMID: 16844935 (full text)
3)Eur J Radiol. 2004 Apr;50(1):67-73.
Blunt trauma to the gastrointestinal tract and mesentery: is there a role for helical CT in the decision-making process?
Scaglione M, de Lutio di Castelguidone E, Scialpi M, Merola S, Diettrich AI, Lombardo P, Romano L, Grassi R.
The CT diagnosis of bowel and mesenteric injuries is difficult and warrants optimal technique and skilled interpretation. We retrospectively reviewed 36 consecutive patients with blunt traumatic injuries to the bowel and mesentery at our regional level I trauma center during the past 3 years. Physical examination, laboratory, Computed tomographic (CT), and intraoperative findings were compared. Surgically proven bowel injuries (13 cases) occurred in the duodenum (three cases), ileum (two cases), jejunum (two cases), colon (three cases), and stomach (three cases). CT findings considered specific of bowel rupture were observed in 5/13 patients including: extraluminal oral contrast or luminal content extravasation (four cases) and discontinuity of hollow viscus wall (one case). In the remaining 8/13 CT findings considered suggestive of bowel injury consisted of: pneumoperitoneum (six), gas bubbles close to the injured hollow viscus (three), thickened (>4-5mm) bowel wall (five), bowel wall hematoma (three), intraperitoneal fluid of unknown source (three). Mesenteric injury (23 cases) were surgically observed at the level of the mesenteric vessels (17 cases), legament of Treitz (two cases), gastro-duodenal artery (one case), transverse (one case) and sigmoid mesocolon (one case). CT finding considered specific of mesenteric laceration was active extravasation of contrast material from the mesenteric vessels (10 cases). CT findings suggestive of mesenteric injury (13 cases) consisted of: mesenteric hematoma (five) and/or high attenuation fluid collections, within the mesenteric root (eight) and folds (four). Helical CT is sensitive in the identification of bowel and mesenteric injury after blunt trauma providing a wide spectrum of findings. However, CT cannot be used as the sole indicator in cases with isolated thichened bowel wall, mesenteric hematoma, bowel hematoma, pneumoperitoneum or gas bubbles. Persistent, active extravasation of intravenous constrast medium from the mesenteric vessels, in isolation or associated with further injuries, requires immediate exploration and repair; disruption of bowel wall and extravasation of oral contrast are definite signs of bowel rupture. Close clinical observation, monitoring, and surgical expertise are mandatory for appropriate management.PMID: 15093237
4)J Trauma. 2001 Jul;51(1):26-36.
Helical computed tomography of bowel and mesenteric injuries
.Killeen KL, Shanmuganathan K, Poletti PA, Cooper C, Mirvis SE.
BACKGROUND: The role of computed tomography in diagnosing hollow viscus injury after blunt abdominal trauma remains controversial, with previous studies reporting both high accuracy and poor results. This study was performed to determine the diagnostic accuracy of helical computed tomography in detecting bowel and mesenteric injuries after blunt abdominal trauma in a large cohort of patients. METHODS: One hundred fifty patients were admitted to our Level I trauma center over a 4-year period with computed tomographic (CT) scan or surgical diagnosis of bowel or mesenteric injury. CT scan findings were retrospectively graded as negative, nonsurgical, or surgical bowel or mesenteric injury. The CT scan diagnosis was then compared with surgical findings, which were also graded as negative, nonsurgical, or surgical. RESULTS: Computed tomography had an overall sensitivity of 94% in detecting bowel injury and 96% in detecting mesenteric injury. Surgical bowel cases were correctly differentiated in 64 of 74 cases (86%), and surgical mesenteric cases were correctly differentiated from nonsurgical in 57 of 76 cases (75%). CONCLUSION: Helical CT scanning is very accurate in detecting bowel and mesenteric injuries, as well as in determining the need for surgical exploration in bowel injuries. However, it is less accurate in predicting the need for surgical exploration in mesenteric injuries alone.PMID: 11468463
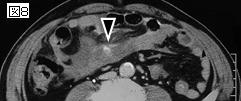
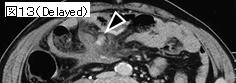
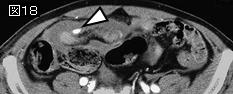
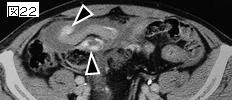
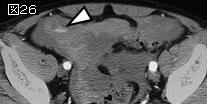
上記文献のまとめ:消化管穿孔のCT所見.
直接所見
1:腸管壁の断裂像(bowel discontinuity),特異度(specificity)は高いが陽性率
(sensitivity)は低い.
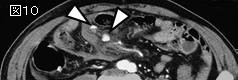
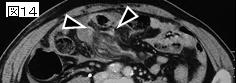
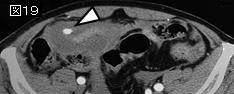
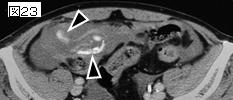
2:遊離ガス(extraluminal air,pneumoperitoneum),陽性率は意外と低く50%前後.特異度は
高いが,消化管穿孔以外の原因もあり慎重な臨床的判断を要する.他の所見が複数加われば消化管穿孔の
可能性は100%に近い.
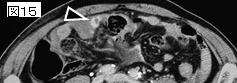
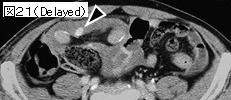
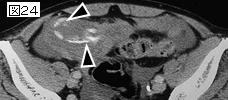
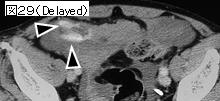
3:経口的に投与した造影剤の腸管外漏出(extraluminal oral contrast material),特異度は最も
高い(100%)が,陽性率は意外と低く(19〜42%),時間がかかる,麻痺性イレウスの症例が多い,
誤嚥の可能性などから敬遠されつつある.
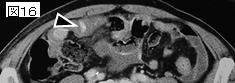
4:腸管内容物の腸管外漏出,
間接所見
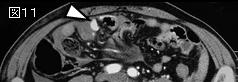
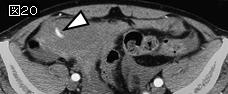
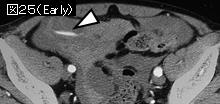
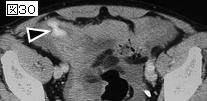
5:腸管壁肥厚(bowel wall thickening).直接打撲,腸間膜損傷による虚血または静脈還流障害
によるものとされる.陽性率は70%前後.連続2スライス以上で3,4mm以上を壁肥厚とする文献が多いが,
腸管の拡張度に影響を受けるのでそう単純ではない.「ある程度の内容物を含み(虚脱していない),
厚さが4mm以上で,周囲の正常な腸管より明らかに壁肥厚を呈する」が適当な読影の仕方と思われる.
壁肥厚だけの単独所見は特異度は高くなく,液貯留(腹水)や遊離ガス,腸間膜の濃度上昇があれば
消化管穿孔の可能性は極めて高くなる.
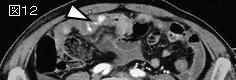
6:腸間膜の濃度上昇.infiltration(境界不鮮明な濃度上昇),stranding(streaking:スジ状の
濃度上昇)などと呼ばれ,血腫,腸液あるいは炎症性の反応を反映するといわれる.70%前後に認め
るが単独では特異度は低い.
7:液貯留・腹水(unexplained free fluid:実質臓器損傷を認めないが液貯留・腹水がある).
陽性率は高く特異度は低いが,小腸間や腸間膜間に存在するものは消化管穿孔や腸間膜損傷を示唆
する.
8:麻痺性イレウス .
|