|
文献考察:脾梗塞後のガス発生
1)Killeen KL, Shanmuganathan K, Boyd-Kranis R, Scalea TM, Mirvis SE
CT findings after embolization for blunt splenic trauma.
J Vasc Interv Radiol. 2001 Feb;12(2):209-14.
PURPOSE: To determine complications after transcatheter embolization for blunt splenic injury as recognized with computed tomography (CT). MATERIALS AND METHODS: From March 1997 to January 2000, 80 patients underwent transcatheter embolization after blunt splenic injury, of whom 53 underwent abdominal CT examination before and after embolization. Preembolization CT scans were reviewed to determine grade of injury, and postembolization CT scans were reviewed to identify complications secondary to embolization. Arteriography results were reviewed to determine findings and method and location of embolization. RESULTS: Splenic infarcts occurred in 63% of patients after proximal embolization and in 100% of patients after distal embolization. Infarcts after distal embolization tend to be larger and occur just distal to the embolization material, whereas infarcts after proximal embolization tend to be smaller, multiple, and located in the periphery. Most infarcts resolved without sequelae. Seven patients developed gas within an infarct or subcapsular fluid collection. Two collections were drained and found to be sterile and one patient had a splenic abscess at laparotomy. CONCLUSIONS: Infarcts are common after splenic embolization. Gas may be present within an infarct after embolization with Gelfoam; however, the presence of air/fluid level is a better predictor of abscess. PMID: 11265885
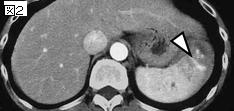
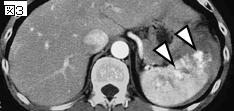
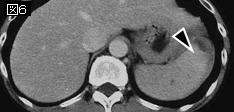
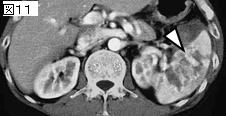
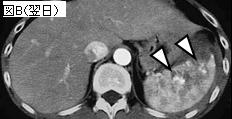
追記:脾梗塞後1〜7日にガスが発生することがある.その機序については説明されていない.感染と間違えないことが大事,被膜下でニボーを形成しているのは膿瘍の可能性が高い.
2)Am Surg. 2003 Dec;69(12):1036-9; discussion 1039-40.
Air following splenic embolization: infection or incidental finding?
Haan J, Bochicchio G, Kramer M, Scalea T.
The use of splenic embolization for nonoperative management has increased. With increased use of this adjunct, a new and frequent finding has been air within the areas of infarction in patients with or without clinical signs of infection. The purpose of this study was to determine if air within areas of splenic infarction is pathologic of infection or rather an incidental finding. A retrospective review over the past 3 years of inpatients undergoing splenic embolization and having pre- and postembolization abdominal computed tomography scans were reviewed for the findings of free air as well as any clinical signs of infection. A total of 96 consecutive patients were included. Of these, 12 had evidence of infarction with air. Six of these patients had undergone distal embolization with intraparenchymal air, but no symptoms. These were successfully observed. Two patients demonstrated subcapsular air/fluid levels, which underwent drainage with splenic preservation. Cultures were negative for infection. The remaining 4 underwent splenectomy. Of these, all had large collections of air. Two of these 4 spleens were infected: 1 with alpha-hemolytic Streptococcus and one with Clostridia perfringens. The remainder was sterile. This gave an overall infection rate of 17 per cent of patients with evidence of air. This yield increased to 33 per cent if the patient had symptoms and 50 per cent in those with large amounts of air and symptoms. Overall, we feel that air following embolization is a concern, but does not constitute infection. Patients with large amounts of air and signs and symptoms of infection will have a far higher infectious rate, 50 per cent in this limited series. In these patients, evaluation for infection is indicated; that being percutaneous sampling versus splenectomy. PMID: 14700287
|