|
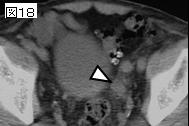
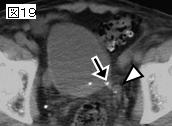
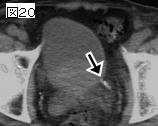
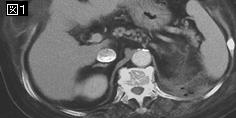
文献考察:腎周囲膿瘍
1)【腎尿路感染症の全て 最近の動向】 腎膿瘍, 腎周囲膿瘍(解説/特集)
Author:諸角誠人(琉球大学 医学部 泌尿器科), 小川由英
Source:腎と透析(0385-2156)55巻1号 Page73-76(2003.07)
2)【感染症症候群(III)】 専門領域別感染症 泌尿器科領域感染症 腎膿瘍, 腎周囲膿瘍(解説/特集)
Author:速見浩士(鹿児島大学 医 泌尿器科), 後藤俊弘, 川原元司, 大井好忠
Source:日本臨床(0047-1852)別冊感染症症候群III Page234-236(1999.03)
3)Schaeffer AJ.
Renal Abscess.in ”Infections of the Urinary Tract”.
Campbell-Walsh Urology,8th Ed, WB Saunders,Philadelphia.558-559,2002.
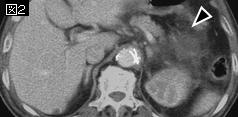
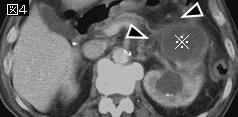
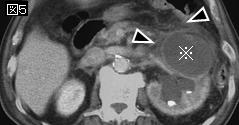
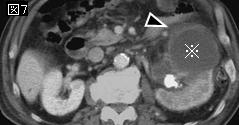
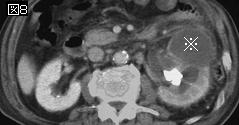
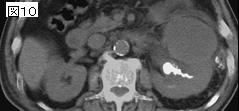
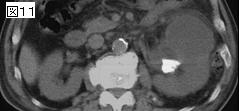
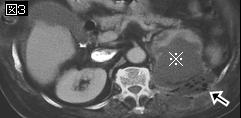
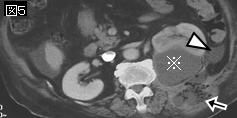
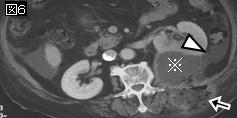
3文献のまとめ.腎周囲膿瘍は腎被膜とGerota筋膜(腎筋膜)との間に形成される膿瘍で,感染部位からの血行性播種(約1/3),あるいは逆行性尿路感染に続く膿腎症や腎膿瘍からの波及により発症する.1/3に糖尿病がみられ,1/3に尿路結石を合併する.起因菌で多いのはE.coli. ProteusとStaphylococcus aureusである.適正な抗生物質投与を行っても5日以上発熱が続く場合は腎盂腎炎よりも腎周囲膿瘍を考慮すべきである.外科的ドレナージ後基礎疾患に対する治療を施行する.
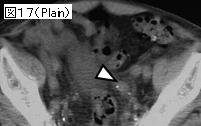
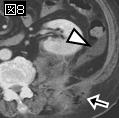
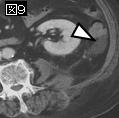
4)3cm以上の膿瘍はドレナージ(図)
J Urol. 2002 Oct;168(4 Pt 1):1337-40.
Current treatment and outcomes of perinephric abscesses.
Meng MV, Mario LA, McAninch JW.
PURPOSE: We characterize the treatment and outcomes of perinephric abscesses in a contemporary cohort of patients. MATERIALS AND METHODS: We reviewed the experience with perinephric abscesses at a single community based hospital. Abdominal computerized tomography (CT) was widely available during the study period and experience with radiographic guided percutaneous drainage was extensive. Therapy and intervention for individual patients were dictated by the treating physician. RESULTS: Of the 25 patients identified with perinephric abscesses 3 (12%) ultimately died. Although 40% had multiple risk factors for perinephric abscesses only 35% were identified at presentation. Urine cultures were positive in 72% of patients and CT had a diagnostic sensitivity of 92%. Ten patients with a mean abscess size of 1.8 cm. were treated with antibiotics alone (mean hospitalization 10 days) while 11 with a mean abscess size of 11 cm. received antibiotics and initial percutaneous drainage (mean hospitalization 30 days). Of the 11 patients treated with percutaneous drainage 4 ultimately required surgical exploration and nephrectomy. CONCLUSIONS: The clinical characteristics of perinephric abscesses have not changed significantly but improved imaging with CT allows earlier diagnosis and treatment, which likely contributed to the reduced mortality in our cohort compared to historical series. With accurate staging and careful followup, a variety of treatments can be successful, including antibiotics alone or in conjunction with percutaneous drainage and urinary drainage. Open surgical drainage and nephrectomy may eventually be required in some patients and should be considered if adequate drainage is not achieved.PMID: 12352387
|











;){kind=link}