|
文献考察:門脈-肝静脈(体循環)シャント(Portal-systemic shunt)
1)AJR Am J Roentgenol. 2003 Jul;181(1):71-8.
Symptomatic intrahepatic portosystemic venous shunt: embolization with an alternative approach.
Tanoue S, Kiyosue H, Komatsu E, Hori Y, Maeda T, Mori H.
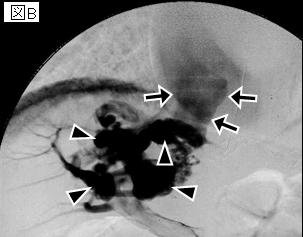
OBJECTIVE: Intrahepatic portosystemic venous shunt is relatively rare and not well recognized. Awareness of intrahepatic communications is important because they can cause encephalopathy, and most of these shunts can be completely cured by transcatheter embolization. In this study, we describe the angiographic findings and transcatheter embolization techniques using several approaches for the treatment of intrahepatic portosystemic venous shunt. MATERIALS AND METHODS: Between 1989 and 2001, we treated 10 patients with symptomatic intrahepatic portosystemic venous shunt by performing transcatheter embolization with Gianturco coils, fibered platinum coils, detachable balloons, and detachable microcoils using one of three approaches to access the portal venous system: transileocolic obliteration (n = 2), percutaneous transhepatic obliteration (n = 4), or retrograde transcaval obliteration (n = 4). RESULTS: In all patients, complete obliteration or nearly complete obliteration was confirmed angiographically, and symptoms related to portal-systemic encephalopathy improved after treatment. Complications were observed in three patients: adhesive ileus in a patient treated by transileocolic obliteration and thrombosis of intrahepatic portal branches in two patients treated by percutaneous transhepatic obliteration. CONCLUSION: On angiography, two types of intrahepatic portosystemic venous shunt were seen: intrahepatic portal venous-hepatic venous communication and intrahepatic portal venous-perihepatic venous communication. Transcatheter embolization is effective for treatment of intrahepatic portosystemic venous shunt. Retrograde transcaval obliteration is the least invasive technique and is recommended as the first choice for treatment of portosystemic venous shunt except in patients with multiple shunts.PMID: 12818832(full text)
2)Br J Radiol. 2003 Jul;76(907):487-90.
Intrahepatic portosystemic venous shunt: diagnosis by colour/power Doppler imaging and three-dimensional ultrasound.
Oguz B, Akata D, Balkanci F, Akhan O.
Intrahepatic portosystemic venous shunt, considered to be a rare disease, can lead to hepatic encephalopathy. With recent advances in diagnostic imaging techniques, the number of reports of intrahepatic portosystemic venous shunts identified incidentally in patients without symptoms are increasing. We report an intrahepatic portosystemic venous shunt that was diagnosed incidentally by real-time ultrasound and colour Doppler imaging, including the use of three-dimensional ultrasound using minimum intensity projections and power Doppler.PMID: 12857710(full text)
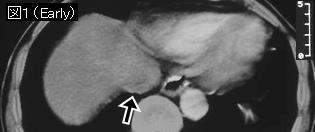
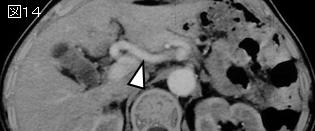
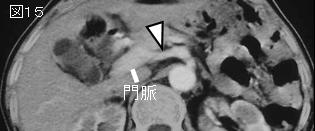
2文献の要旨:肝硬変から門脈圧亢進症が発生し,門脈体循環短絡路(portosystemic shunt)が形成され肝性脳症を発症することはよく知られているが,肝硬変のない門脈体循環短絡路はまれである.先天性と後天性に分類され,後天性の原因としては外傷,門脈瘤の破裂などがいわれている.また肝内門脈体循環短絡路は先天性で,門脈肝周囲(肝外)静脈短絡路は門脈圧亢進症が原因である場合が多い.脳細胞のアンモニアに対する耐性が低下する50歳台以後に発見される症例が多い.
|