|
文献考察:肝エキノコックス症(hepatic echinococcosis).
1)【肝良性疾患 鑑別診断と治療法選択のupdate】 寄生虫性肝嚢胞
Author:紀野修一(旭川医科大学 第2外科), 葛西眞一
Source:臨床外科(0386-9857)56巻7号 Page893-901(2001.07)
Abstract:寄生虫疾患で肝に嚢胞性病変をきたす可能性のある疾患として, 肝包虫症, アメーバ性肝膿瘍, 肝吸虫症, 肝蛭症が挙げられる. 最も遭遇する可能性が高い多包虫症は, 北海道の風土病と思われているが, 北海道以外でも患者が発生している. 又, 本症は進行すると肝悪性腫瘍に似た病態をとり, 肺, 脳等に転移性病巣を作るが, 有効な化学療法が施行できるため, 正確に診断し治療することが重要である. 肝腫瘤性病変や嚢胞性病変で, 日常経験する腫瘍や嚢胞と比較して非典型的な所見を呈する場合は, 本症に特異的な血清診断を行い治療前に確定診断を得ることが大切である.
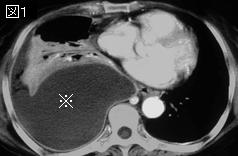
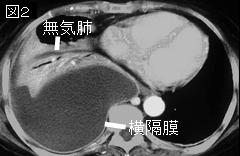
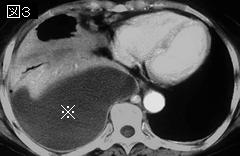
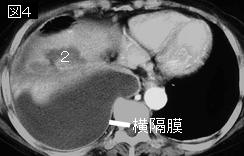
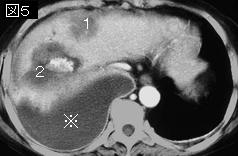
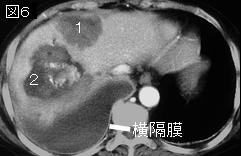
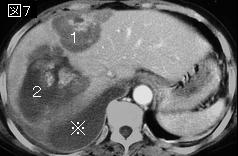
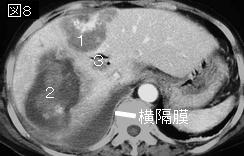
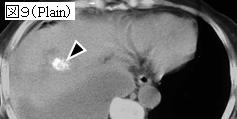
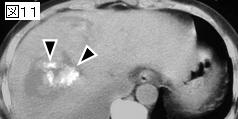
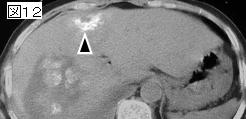
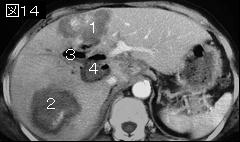
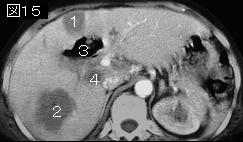
要旨:肝包虫症はエキノコックスの幼虫が肝に嚢胞性病変をきたす疾患で,1)単包条虫{Echinococcus granulosus)の感染による単包虫症(granular echinoccocosis, cytic hydatid disease)と, 2)多包条虫(Echinococcus multilocularis)の感染による多包虫症(alveolar echinococcosis, alveolar hydatid disease)の2つに分けられる.単包虫症はは現在は国内での感染例はないとされるが,多包虫症は北海道を主として発生している.終宿主であるイヌやキツネとの接触や,虫卵が付着した食物の経口摂取により感染する.腸管内で虫卵は孵化し幼虫となり,門脈を介して肝に達する.病態からみた病期は表1,WHOの病期分類は表2.多包虫症のWHOの治療ガイドラインでは,1)手術可能な病変では切除が第1選択で,術後一定期間の化学療法(アルベンダゾール)を行うこと,2)切除不能な病変や非完全切除例では長期の化学療法が適応としている.
しかし,下記文献のように縮小手術や,PAIR療法:(percutaneous puncture,aspiration,injection:albendazoleまたは高張生食水,reaspiration)を推奨する文献もある.
2)Arch Surg. 2006 Nov;141(11):1101-8.
Hydatid disease of the liver: a continuing surgical problem.
Safioleas MC, Misiakos EP, Kouvaraki M, Stamatakos MK, Manti CP, Felekouras ES.
HYPOTHESIS: To study the results of different surgical strategies in the treatment of liver hydatid disease. DESIGN: A retrospective study of 287 patients. SETTING: A university hospital in Athens, Greece. PATIENTS: Two hundred eighty-seven patients with liver hydatid cysts treated surgically 1977-2004. The cysts were located in the right hepatic lobe in 192 cases, in the left lobe in 66 cases, and in both lobes in 29 cases. Eleven patients had concomitant cysts in other organs and 12 patients had multiple intra-abdominal cysts. RESULTS: All patients were treated surgically. Surgical procedures included external drainage, simple closure, marsupialization, partial cystectomy with omentoplasty, radical procedures, laparoscopic drainage, and radiofrequency ablation. The first 3 techniques carried a higher complication rate (36.5%) compared with the other techniques (17.85%; P<.05 however omentoplasty and external drainage carried a higher recurrence rate overall as compared with radical procedures conclusion: carry lower complication the formerly used marsupialization drainage. conservative techniques such other offer an effective control of hepatic hydatidosis are preferred over when possible.pmid:>
3)Clin Radiol. 2000 Nov;55(11):839-48.
Percutaneous drainage of hydatid cyst in the liver as a primary treatment: review of 52 consecutive cases with long-term follow-up.
Bosanac ZB, Lisanin L.
AIM: To evaluate the suitability of percutaneous drainage as a primary and definitive treatment of hydatid disease of the liver. MATERIALS AND METHODS: Between October 1989 and April 1992, percutaneous drainage was performed on 52 consecutive patients (27 women and 25 men aged 13 to 84 years) with 55 hydatid cysts in the liver. Twenty-five (45%) cysts were type I, 10 (18%) were type II, 14 (25%) were type III, 5 (10%) were type IV and 1 (2%) was type V. All procedures were performed under light sedation and local anaesthetic at the puncture site. The standard Seldinger technique was used. Initial puncture was performed under ultrasound (US) guidance through the liver parenchyma. The rest of the procedure was conducted under fluoroscopic control. Pigtail drainage catheters (size 12-20 Fr) were used, with Betadine (10% povidone iodine; 1% free iodine) being allowed to act within the cyst for 30 min, as a scolicidal agent. RESULTS: All the patients were successfully treated and 6-9 year follow-up involving US, computed tomography (CT) and serology tests showed no local recurrence or spread of the disease. No major (death, cyst rupture, anaphylactic shock) and very few minor complications arose. Two patients had mild skin reaction with nausea requiring no treatment and three patients developed a secondary infection of the cyst, due to prolonged drainage time. These liver abscesses responded successfully to further catheter drainage. Subsequent patients were treated with large bore (18-20 Fr) catheters and none developed secondary infection. Overall drainage time varied from 7-118 days (7-28 days, if we exclude three initial cases who had prolonged drainage). CONCLUSION: It is our strong belief that percutaneous drainage using the above method should be considered a first-line treatment for hydatid disease of the liver.Bosanac, Z. B., Lisanin, L. (2000). Clinical Radiology55, 839-848. Copyright 2000 The Royal College of Radiologists.PMID: 11069739
|








;){kind=link}
;){kind=link}