|
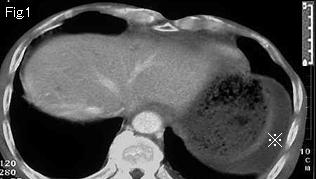
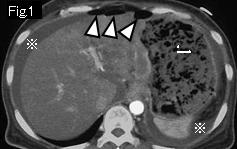
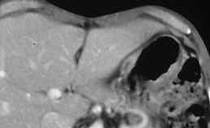
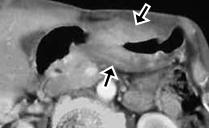
Reference case 1 (5mm slice, gastric cancer perforation): A 53-year-old female with schizophrenia. Over one month, she developed appetite loss, anemia, and gradually distending abdomen. She presented with increasing epigastric pain for several hours. Temperature: 37.5 degrees Celsius, abdomen showed signs of generalized peritonitis.
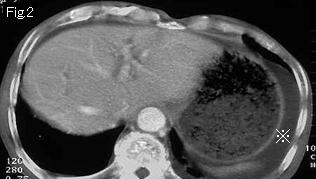
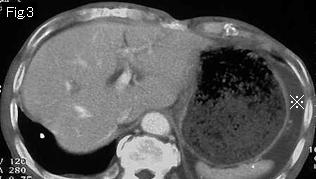
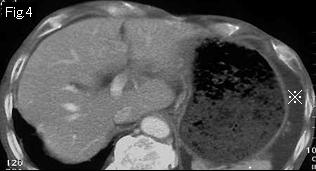
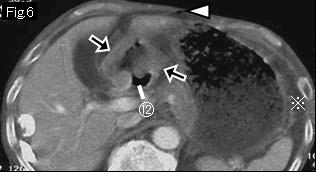
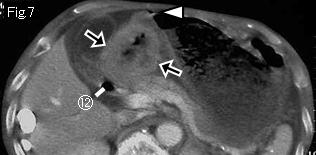
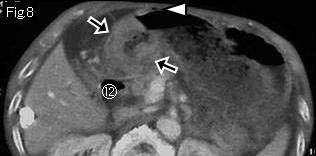
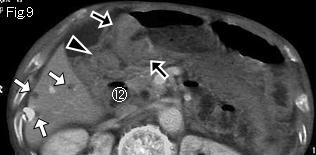
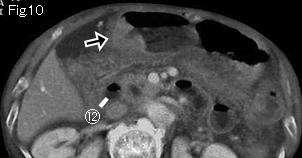
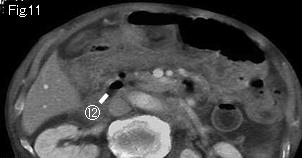
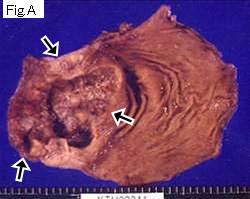
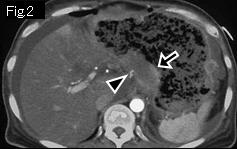
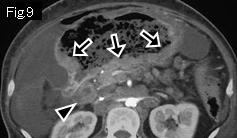
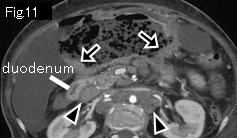
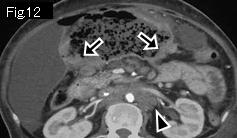
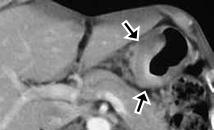
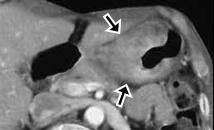
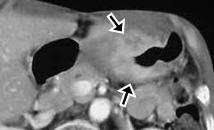
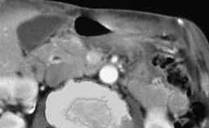
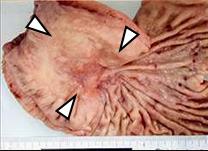
Ascites (reference mark) and free air (white arrowheads) in Fig.1 indicate gastrointestinal perforation. Stomach is dilated with food residue. Black arrows in Fig.2-Fig.12 show contrast-enhanced wall thickening in comparison with the other part, and black arrowheads are enlarged lymph nodes, which leads to a diagnosis as perforation of advanced gastric cancer. Surgery and pathological examination revealed perforation of gastric cancer with extensive invasion into retroperitoneum.
|