|
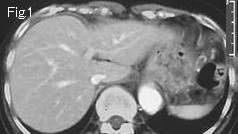
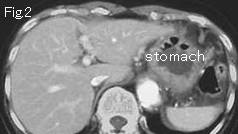
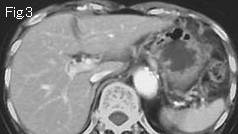
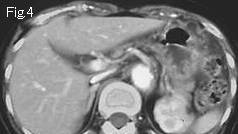
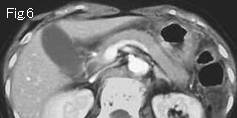
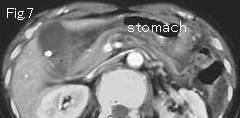
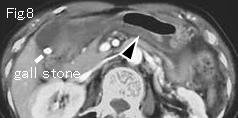
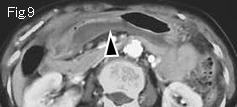
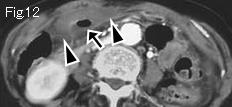
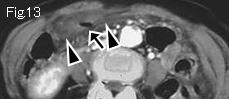
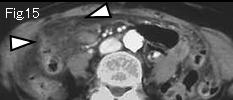
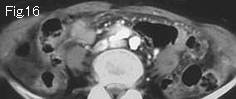
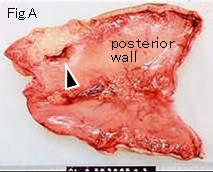
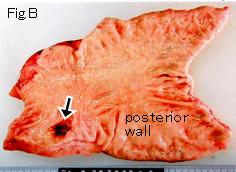
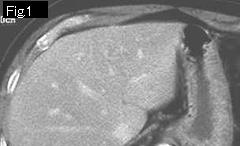
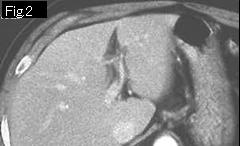
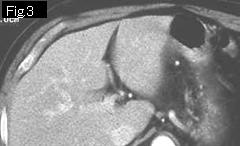
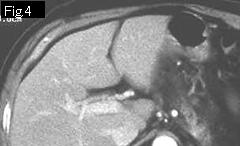
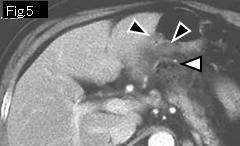
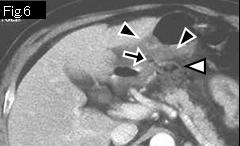
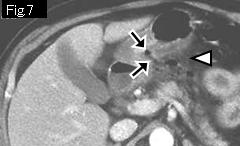
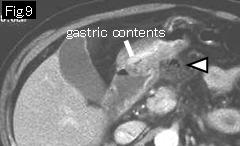
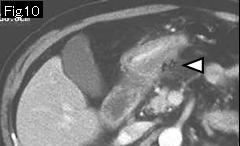
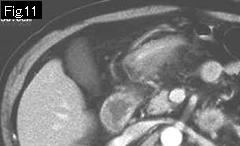
Reference case: (gastric ulcer perforation): A 57-year-old male with a past history of duodenal ulcer 9 years ago, presented with gradually aggravating epigastric pain for 24 hours. Temperature: 36.7 degrees Celsius. There is tenderness in epigastrium. No free air is seen directly beneath the anterior abdominal wall. In Fig.1-Fig.4, gastric wall does not show submucosal edema to indicate an acute lesion. Pyloric wall manifests submucosal edema from Fig.5 (black arrowhead), and Fig.6-Fig.8 show gas and defect (black arrow) in the posterior wall that is thickened by submucosal edema. Note that free air and food debris (white arrowhead) in omental sac of Fig.5-Fig.10 are depicted. As a result, diagnosis as perforation of ulcerative lesion of pyloric posterior wall of stomach can be made. Fig. C is resected specimen and pathology reported as benign gastric ulcer with perforation.
|